

Copyrights: Yousef Khani, Masoumeh Arabsalmani, Reza Pakzad, Mahshid Ghoncheh, Abdollah Mohammadian-Hafshejani, Hamid Salehiniya, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Pancreatic cancer (PC) is as the twelfth most frequent cancer and the seventh most important cause of mortality by reason of cancer in the world. Being informed about the incidence and mortality of this cancer and the potential role of development is useful in health policy. The aim of this research is investigating disparities in the incidence and mortality of PC in the world countries in the year 2012.
Methods: This study was an ecologic study in the World for assessing the correlation between Human Development Index (HDI) and its details (Gross national income (GNI) per capita, average years of schooling and life expectancy at birth) with age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) of PC.
Results: In total, 337872 new cases of PC occurred in 2012 around the world , that 178116 and 159711 cases take happen in men and women respectively, also at the same year 330391 deaths of PC occurred ,that 173,827 and 156564 cases were in men and women. In assessment the relationship between HDI and ASIR and ASMR of PC there is significant positive correlation equal to 0.767 (p <0.001) between HDI and ASIR of PC, and a significant positive correlation equal to 0.776 (p <0.001) between HDI and ASMR of PC.
Conclusion: The incidence and mortality of PC has a significant positive correlation with the Human Development Index.
Introduction
Gastrointestinal cancers have high incidence and mortality rate worldwide Jemal et al., 2010aSiegel et al., 2012. pancreatic cancer (PC) is one of the cancers that is identified as the twelfth common cancer and the seventh death cause due to cancer worldwide so that its incidence was 12.2 and death due to that was 10.9 per hundred thousand people in 2014 Howlader et al., 2011. The highest incidence of PC is observed in Northern Europe and America and the lowest incidence is seen in African countries Altekruse et al., 2010Curado et al., 2007Malvezzi et al., 2013Pakzad et al., 2016. Totally, 2/3 of PC death cases occur in world developed countries Parkin et al., 2005. Therefore it's known as the fifth deadly cancer in developed countries in 2000 Schwartz and Reis, 2000.
Despite the diagnosis of more than 400000 PC new cases in year, it is about 30 years that its 5-year survival remains low and less than 4 percent is reported for this cancer Baxter et al., 2007Jemal et al., 2010bStats, 2012. The global burden of PC is increasing due to aging, population growth and high-risk behaviors especially smoking and world developed countries allocated the greatest burden of the disease Jemal et al., 2011. As the country is more advanced and has higher-income, non-communicable diseases such as cancers include more death causes Mathers et al., 2005. However, the cause of incidence and prevalence of PC is due to its risk factors including age over 70, smoking, race, obesity, alcohol, red and processed meat consumption, chronic pancreatitis, diabetes and chronic infections (hepatitis B, hepatitis C, Helicobacter pylori) different distribution that is believed to be higher in developed countries Keane et al., 2014Lowenfels and Maisonneuve, 2006Society, 2013. The society health is the outcome of several complex, different and constantly changing factors Organization, 2000. So, it should be cared, intervened and managed and be in the place of social and economic development level, continuously Organization, 2000. Therefore, one of the good public health and its related factors indicator is the Human Development Index (HDI) Bray et al., 2012. This index is a useful classification for cancer globalization Bray et al., 2012. The HDI was determined as a comparing index for countries in 3 fields of human dimension by the UNDP (United Nations Development Program) in 1990 Ravallion, 1997. Three dimensions of HDI include long and healthy life, access to knowledge and good living standards Bray et al., 2012. Each of these factors are measured by life expectancy at birth, education and GDP per capita, respectively Bray et al., 2012.
An estimated 5-year incidence of all cancers according to HDI regions showed that areas with high and very high HDI, have allocated highest prevalence of 21.31% to themselves despite having only 6.1% of the world's population and this ratio was 9.237% and 1.993 % for medium and low HDI regions, respectively Bray et al., 2013.
PC among other cancers has different incidence and mortality that varies around the world and it is due to development and the diagnostic and therapeutic status of countries Bray, 2014Forman et al., 2014Franceschi and Wild, 2013Kanavos, 2006.
However, a comprehensive study that could examine the association between HDI and age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) of PC has not been conducted. Because of this point that knowledge about the ASIR and ASMR of cancers and the potential role of development is useful in health planning, this study conducted with the purpose of determining the ASIR and ASMR of PC and its correlation with the HDI in the world in 2012.
Materials-Methods
This study was an ecologic study in the World for assessing the correlation between HDI and its details (Gross national income (GNI) per capita, average years of schooling and life expectancy at birth) with age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) of PC. Detailed descriptions of the methods used in collection of data about cancer incidence and mortality in GLOBOCAN Ferlay J et al., 2016, and HDI Malik, 2013, and Statistical analysis of this study have been provided in previous reports Arabsalmani et al., 2017Ghoncheh et al., 2016Hassanipour-Azgomi et al., 2016Mohammadian et al., 2017Mohammadian et al., 2016Rafiemanesh et al., 2016Razi et al., 2016Shuja et al., 2017Tiyuri et al., 2017.
Results
The frequency of incidence of PC
In total, 337872 PC cases have been occurred worldwide in 2012 that 178161 and 159711 cases were in men and women respectively (Sex Ratio = 1.11). From all occurred cases, about 174344 cases were in countries with very high HDI, 55638 cases were in countries with high HDI, 98632 cases were in countries with medium HDI, and 9108 cases occurred in countries with low HDI. Five countries with the heights sum of PC include: China (65727), America ( 42885),Japan (32899), Germany (16451) and Russia (14512). five countries with highest sum of PC case in men include: China (39299), America (21713), Japan (17013), Germany (7972) and Russia (7206), and in women include: China (26428), America (21172), Japan (15886), Germany (8479), and Russia (7306).
The ASIR of PC
The ASIR of PC per hundred thousand people in the world was 4.2 (in men 4.9 and in women 3.6). The ASIR of PC in very high HDI regions was 7.2, in high HDI regions was 4.6, in medium HDI regions was 2.7, and in low HDI regions was 1.2. Five countries with the highest ASIR of PC are: Czech Republic (9.7), Slovakia (9.4), Armenia (9.3), Hungary (9.3), and Slovenia (8.8), respectively. 5 countries with the highest ASIR of PC for men were: Armenia (11.9), Czech Republic (11.9), Slovakia (11.5), Hungary (11.5), and FYR Macedonia (11.5), and in women include: Czech Republic (7.9), Slovenia (7.8), Slovakia (7.8), Denmark (7.7), and Finland (7.6).
The frequency of mortality of PC
Nowadays, 330391 deaths happened because of PC around the world in 2012 that about 173827 cases were men and 156564 cases were women (Sex Ratio = 1.11). Total number of mortality from PC was 170497 cases in very high HDI region, 56474 cases in high HDI region, 94447 cases medium HDI region, and 8822 cases in low HDI region. Five countries having the highest ASMR of PC were: China (63662), America (41509), Japan (31046), Russia (16371), and Germany (16188). Five countries having the highest ASMR of PC in men were: China (37775) cases, America (21005), Japan (15809), Russia (8168), and Germany (7900), and in women include: China (25887), America (20504), Japan (15237), Germany (8288), and Russia (8203).
The ASMR of PC
The ASMR of PC per hundred thousand people in the world was 4 (in men 4.7 and in women 3.4). The ASMR of PC very high HDI regions was 6.8, in high HDI regions was 4.6, in countries with medium HDI regions was 2.6, in low HDI regions was 1.2. Five countries having the highest ASMR of PC per hundred thousand people were: Armenia (8.9), Hungary (8.8), Czech Republic (8.7), Slovakia (8.5), and French Guiana (8.1). Five countries having the highest ASMR of PC in men were: YR Macedonia (11.8), Armenia (11.6), Hungary (11.1), Estonia (10.6), and Latvia (10.4), and in women include: Slovakia (7.6), Czech Republic (7.2), Slovenia (7.2), Hungary (7), and French Guiana (7).
The association between the ASIR of PC and the HDI
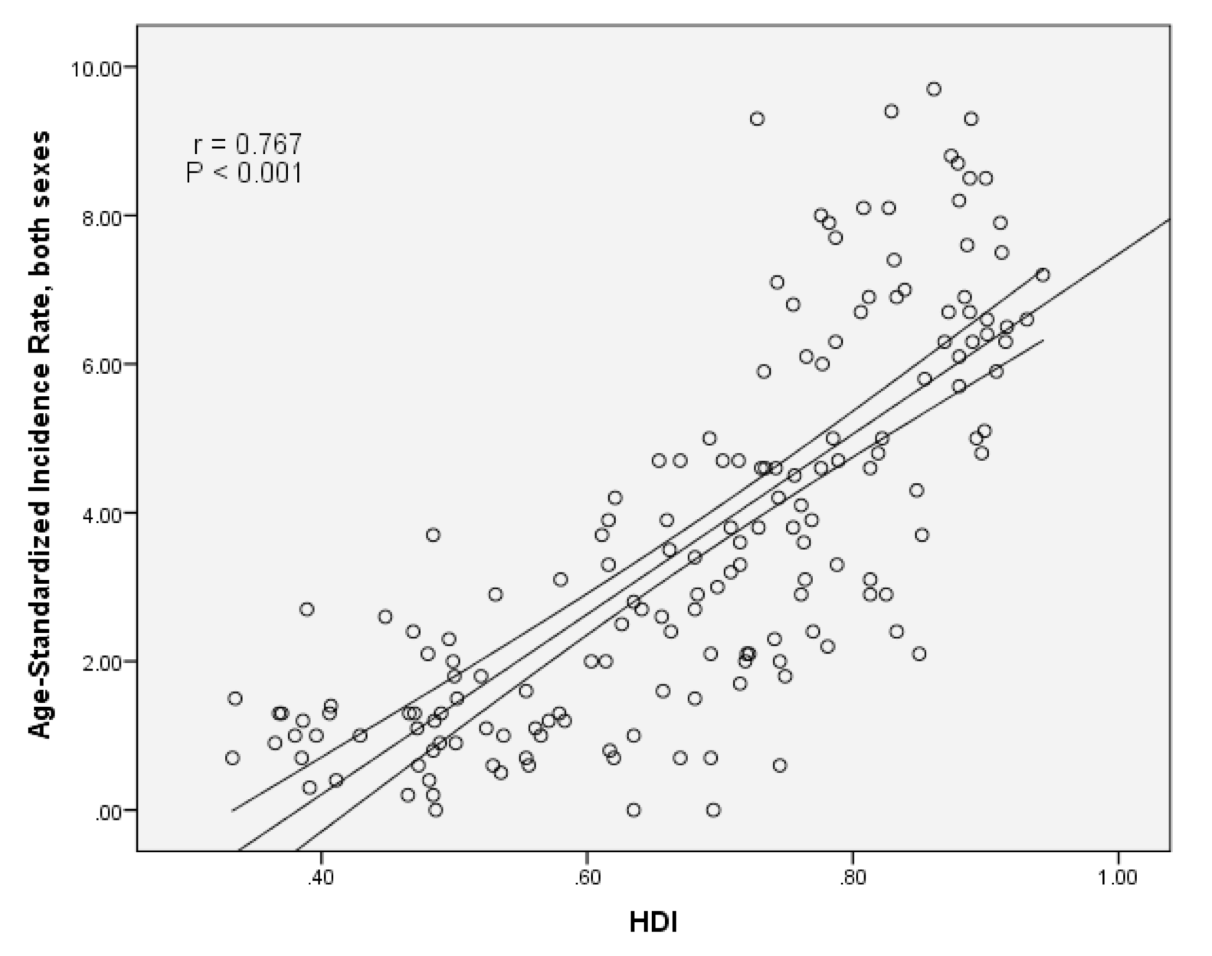
In assessment the relationship between ASIR of PC and the HDI, a significant positive correlation equal to 0.767 (p <0.001) was observed. There were positive correlation between ASIR of PC and components of the HDI (with the level of income equal to 0.517 (p<0.001), with average years of education equal to 0.762 (p<0.001) and with life expectancy at birth equal to 0.657 (p <0.001) ( Figure 1 ).
The association between the ASMR of PC and the HDI
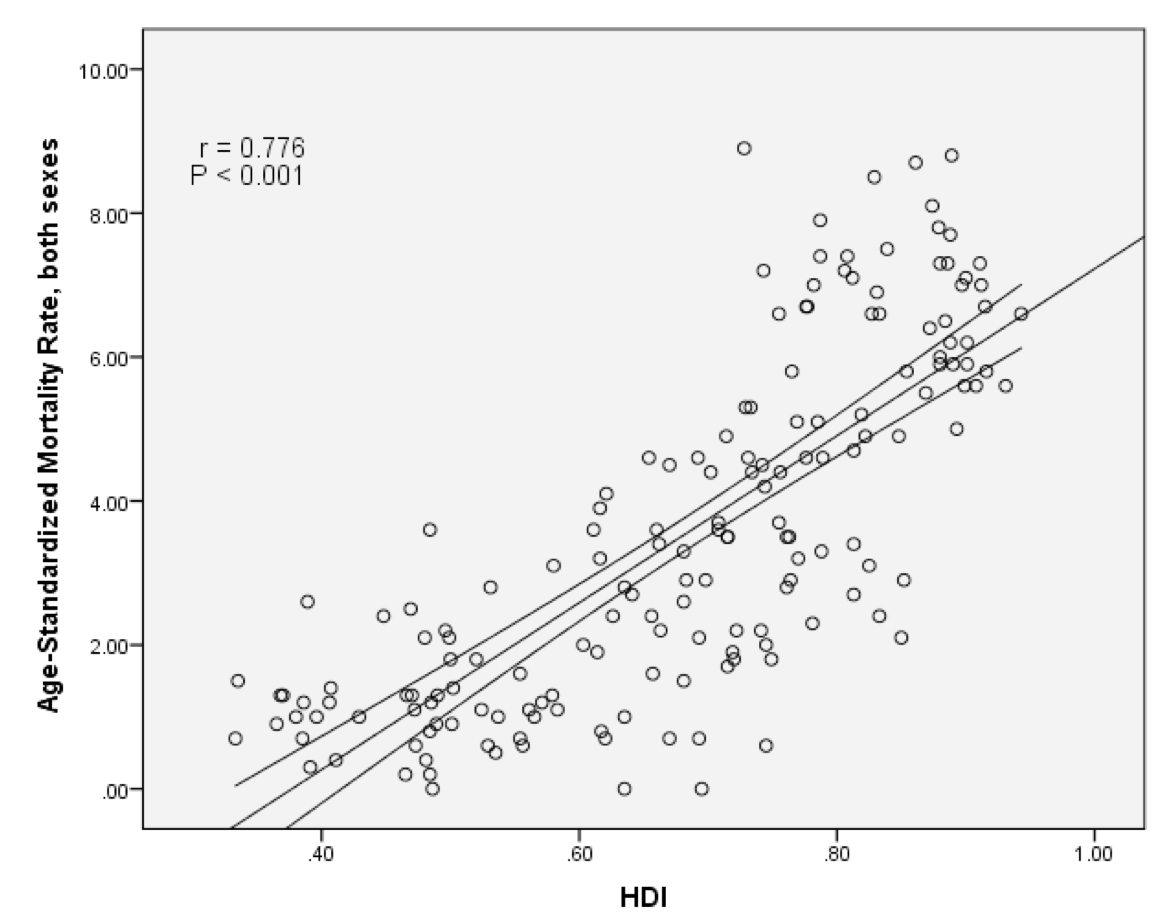
In topic of the relationship between ASMR of PC and the HDI, a significant positive correlation equivalent to 0.776 (p <0.001) was observed. There were positive correlation between ASMR of PC and components of the HDI (with the level of income equal to 0.518 (p<0.001), with average years of education equal to 0.769 (p<0.001) and with life expectancy at birth equal to 0.666 (p <0.001) ( Figure 2 ).
Discussion
PC has allocated the mortality rate of 39.4 and incidence rate of 54.9 cases per 100,000 people of the population to itself in 2008 Hu et al., 2013. Also, according to a cohort study that has been conducted in 2000-2010, incidence of PC has increased 3% annually Keane et al., 2014.
In this study, ASIR of PC was estimated 4.2 per hundred thousand people in the world and has a positive correlation of 0.767 with the HDI that this association is statistically significant. Czech Republic, Slovakia, Armenia, Hungary and Slovenia were 5 countries that allocated the highest rate of incidence to them. This is in condition that every five country is located in group of countries with high and very high HDI.
According to studies, the incidence of PC in industrial developed countries is more than developing ones. In a systematic study which Rio conducted in 1975-2007, it's estimated that the highest incidence of PC belongs to Northern Europe and America Altekruse et al., 2010. Estimating incidence age specified rates (ASRs) is 10.1 for both sexes per hundred thousand people based on gender in Europe in 2012 Ferlay et al., 2013. While, the same rate is estimated to be 3.2 per hundred thousand people in Asia in 2012 Pourhoseingholi et al., 2014.
The diseases incidence is associated with their risk factors Ward et al., 2004. Age and smoking are strong factors that always are reported Bonelli et al., 2003Fuchs et al., 1996Hassan et al., 2007Hippisley-Cox and Coupland, 2012Larsson et al., 2005Muscat et al., 1997Silverman et al., 1994Stapley et al., 2012Valean et al., 2015. So that by increasing the number of years of life that passes by smoking cigarettes, the risk to catch PC also boost per person Keyghobadi et al., 2015. Variety diet could be mentioned that other risk factors. Also several studies have shown that the total amount of calorie and probably fat increase in the diet and obesity, may arise the risk of PC (Ghadirian et al., 1990). Finally, we can say that the high level of these factors in developed countries has led to a greater incidence of PC.
The ASMR of PC was 4 per hundred thousand people in the world in this study and a positive correlation of 0.776 was seen between ASMR of PC and the HDI that this was statistically significant. 5 countries having the highest ASMR of PC are: Armenia, Hungary, Czech Republic, Slovakia, and French Guiana. So that Armenia and French Guiana are located in group of countries with high HDI and three other ones in countries with very high HDI.
Also, due to the results of studies that have been conducted between the years 1993-95, it's estimated that PC was the sixth cause of death among cancers in the United States of America and the United Kingdom Berman, 1995Gold and Goldin, 1998. Also in 2002, according to cancer mortality in the world, the incidence of PC is estimated to be 6-8 per 100 thousand people in men and 4-6 per 100 thousand people in women in developed countries such as Australia and Japan Parkin et al., 2005.
In many Asian countries such as Korea, Singapore and China that have a high HDI, PC mortality is high too Parkin et al., 2005Wang et al., 2003.
In this study, the incidence in men is 4.9 and in women is 3.6 per hundred thousand people and the mortality is 4.7 for men and 3.4 per hundred thousand in women.
However, in all cancer centers an association is reported between PC and gender Bramhall et al., 1995. The prevalence of this disease in men is more than women Bramhall et al., 1995. So that due to global estimation in 2012, the rate of mortality to incidence of cancer in both sexes is almost close (0.94 / 0.97)Valean et al., 2015. Although the incidence in men is generally a little more than women, the high incidence and mortality of PC in men has a variety of causes such as increase in smoking Muniraj et al., 2013, diet (high fat and protein, low fruit and vegetable consumption), consumption of coffee, alcohol and Job hazards (insecticides, aluminum, nickel and acrylamide) that these things cases are seen more in men's lifestyle Greene et al., 2008Lowenfels et al., 1997. While, elevated estrogen in women acts as a death cause lowering agent of PC Greene et al., 2008.
In this study, a positive correlation was observed between the ASIR and ASMR of PC and life expectancy at birth. Also it has been seen in several studies that with increasing age, the incidence of PC dramatically raised up increases Ferlay et al., 2015Hartwig et al., 2009; Neesse et al., 2010; Sasson et al., 2002Toriola et al., 2014. So that the cause for increasing incidence of this cancer in developed countries, may be a reflection of aging Pakzad et al., 2015cSmith et al., 2009. In this study, a significant positive correlation was seen between the ASIR and ASMR of PC with mean education level. Also in Bosetti et al study, the incidence is increased with increasing level of education Bosetti et al., 2012. Also about the PC mortality, the mortality is increased in less educated individuals with age under 15 years Jemal et al., 2013.
In this study, a significant positive correlation was seen between the ASIR and ASMR of PC with average income level. According to several studies, patients with high socio-economic status and PC have good chance for surgical treatment but has no significant impact on patient survival Bakens et al., 2015Michaud, 2004Pakzad et al., 2015a, b. Surgery as the only treatment option for long-term survival in patients with PC as an indicator of the impact of social and economic inequality, is a good witness that socioeconomic status has the lowest effect on patient's survival Bakens et al., 2015Michaud, 2004. Because the average survival of PC is 3-6 months since diagnosis without treatment that has up to 23 months increase after surgery and adjunctive therapies Neoptolemos et al., 2001Neoptolemos et al., 2010. That's why we can say that the incidence of PC is near to its mortality rate Michaud, 2004Ryu et al., 2010. Although in several studies observed that patients with higher income have more improvement than others, but this improvement is very low. Therefore, we cannot consider its protective effects very important Neoptolemos et al., 2001Neoptolemos et al., 2010.
Conclusion
We can say that, the incidence and mortality of PC has a significant positive correlation with the Human Development Index and its components.
Abbreviations
ASIR: Age-Standardized Incidence Rate
ASMR: Age-Standardized Mortality Rate
HDI: Human Development Index
PC: Pancreatic cancer
Author Contribution
All authors contributed to the design of the research. Y KH, M A , R P, and M GH extracted the data and summarized it. All authors drafted the first version. Y KH, A MH and HS edited the first draft. All authors reviewed, commented and approved the final draft.
References
-
S. F.
Altekruse,
C. L.
Kosary,
M.
Krapcho,
N.
Neyman,
R.
Aminou,
W.
Waldron,
H.
Cho.
SEER cancer statistics review, 1975-2007 (p. 7). Bethesda, MD: National Cancer Institute.
2010
.
-
M.
Arabsalmani,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
F.
Hadadian,
F.
Towhidi,
K.
Vafaee,
H.
Salehiniya.
Incidence and mortality of kidney cancers, and human development index in Asia; a matter of concern. Journal of Nephropathology.
2017;
6(1)
:
30-42
.
View Article PubMed Google Scholar -
M.
Bakens,
Y.
van Gestel,
M.
Bongers,
V.
Lemmens,
I.
de Hingh.
Socio-economic status influences chance of undergoing surgical treatment for pancreatic cancer in The Netherlands. Pancreatology.
2015;
15(3)
:
S101
.
View Article Google Scholar -
N. N.
Baxter,
B. A.
Whitson,
T. M.
Tuttle.
Trends in the treatment and outcome of pancreatic cancer in the United States. Annals of Surgical Oncology.
2007;
14(4)
:
1320-1326
.
View Article PubMed Google Scholar -
P. M.
Berman.
Gastroenterology: Clinical Science and Practice. Journal of the American Medical Association.
1995;
274(1)
:
79-79
.
View Article PubMed Google Scholar -
L.
Bonelli,
H.
Aste,
P.
Bovo,
G.
Cavallini,
M.
Felder,
R.
Gusmaroli,
V.
Pugliese.
Exocrine pancreatic cancer, cigarette smoking, and diabetes mellitus: A case-control study in northern Italy. Pancreas.
2003;
27(2)
:
143-149
.
View Article PubMed Google Scholar -
C.
Bosetti,
E.
Lucenteforte,
D. T.
Silverman,
G.
Petersen,
P. M.
Bracci,
B. T.
Ji,
C.
La Vecchia.
Cigarette smoking and pancreatic cancer: An analysis from the International Pancreatic Cancer Case-Control Consortium (Panc4). Annals of Oncology : Official Journal of the European Society for Medical Oncology.
2012;
23(7)
:
1880-1888
.
View Article PubMed Google Scholar -
S. R.
Bramhall,
W. H.
Allum,
A. G.
Jones,
A.
Allwood,
C.
Cummins,
J. P.
Neoptolemos.
Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: An epidemiological study. British Journal of Surgery.
1995;
82(1)
:
111-115
.
View Article PubMed Google Scholar -
F.
Bray.
Transitions in human development and the global cancer burden. World cancer report.
2014;
2014
:
54-68
.
-
F.
Bray,
J. S.
Ren,
E.
Masuyer,
J.
Ferlay.
Global estimates of cancer prevalence for 27 sites in the adult population in 2008. International Journal of Cancer.
2013;
132(5)
:
1133-1145
.
View Article PubMed Google Scholar -
F.
Bray,
A.
Jemal,
N.
Grey,
J.
Ferlay,
D.
Forman.
Global cancer transitions according to the Human Development Index (2008-2030): A population-based study. The Lancet. Oncology.
2012;
13(8)
:
790-801
.
-
M.-P.
Curado,
B.
Edwards,
H. R.
Shin,
H.
Storm,
J.
Ferlay,
M.
Heanue,
P.
Boyle.
Cancer incidence in five continents (Vol. IX). IARC Press, International Agency for Research on Cancer.
2007
.
-
J.
Ferlay,
I.
Soerjomataram,
R.
Dikshit,
S.
Eser,
C.
Mathers,
M.
Rebelo,
D.M.
Parkin,
D. Bray
Forman.
GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://globocan.iarc.fr, accessed on 2/2/2016.
2016
.
-
J.
Ferlay,
E.
Steliarova-Foucher,
J.
Lortet-Tieulent,
S.
Rosso,
J.W.W.
Coebergh,
H.
Comber,
D. Bray
Forman.
Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. European Journal of Cancer.
2013;
49(6)
:
1374-1403
.
View Article PubMed Google Scholar -
J.
Ferlay,
I.
Soerjomataram,
R.
Dikshit,
S.
Eser,
C.
Mathers,
M.
Rebelo,
D.M.
Parkin,
D. Bray
Forman.
Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer.
2015;
136(5)
:
E359-E386
.
View Article PubMed Google Scholar -
D
Forman,
J
Ferlay,
BW
Stewart,
CP.
Wild.
The global and regional burden of cancer. World cancer report.
2014;
:
16-53
.
-
S.
Franceschi,
C. P.
Wild.
Meeting the global demands of epidemiologic transition - the indispensable role of cancer prevention. Molecular Oncology.
2013;
7(1)
:
1-13
.
View Article PubMed Google Scholar -
C.S.
Fuchs,
G.A.
Colditz,
M.J.
Stampfer,
E.L.
Giovannucci,
D.J.
Hunter,
E.B.
Rimm,
W.C. Speizer
Willett.
A prospective study of cigarette smoking and the risk of pancreatic cancer. Archives of Internal Medicine.
1996;
156(19)
:
2255-2260
.
View Article PubMed Google Scholar -
P.
Ghadirian,
J. P.
Thouez,
C.
PetitClerc.
International comparisons of nutrition and mortality from pancreatic cancer. Cancer Detection and Prevention.
1991;
15(5)
:
357-362
.
PubMed Google Scholar -
M.
Ghoncheh,
M.
Mohammadian,
A.
Mohammadian-Hafshejani,
H.
Salehiniya.
The Incidence and Mortality of Colorectal Cancer and Its Relationship With the Human Development Index in Asia. Annals of Global Health.
2016;
82(5)
:
726-737
.
View Article PubMed Google Scholar -
E. B.
Gold,
S. B.
Goldin.
Epidemiology of and risk factors for pancreatic cancer. Surgical Oncology Clinics of North America (PMID:9443987).
1998;
7(1)
:
67-91
.
-
Michael F
Greene.
Creasy and Resnik's maternal-fetal medicine: principles and practice. Elsevier Health Sciences.
2008
.
-
W.
Hartwig,
T.
Hackert,
U.
Hinz,
M.
Hassenpflug,
O.
Strobel,
M. W.
Büchler,
J.
Werner.
Multivisceral resection for pancreatic malignancies: Risk-analysis and long-term outcome. Annals of Surgery.
2009;
250(1)
:
81-87
.
View Article PubMed Google Scholar -
M. M.
Hassan,
M. L.
Bondy,
R. A.
Wolff,
J. L.
Abbruzzese,
J.-N.
Vauthey,
P. W.
Pisters,
D.
Li.
Risk factors for pancreatic cancer: Case-control study. The American Journal of Gastroenterology.
2007;
102(12)
:
2696-2707
.
View Article PubMed Google Scholar -
S.
Hassanipour-Azgomi,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
F.
Towhidi,
S.
Jamehshorani,
H.
Salehiniya.
Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate International.
2016;
4(3)
:
118-124
.
View Article PubMed Google Scholar -
J.
Hippisley-Cox,
C.
Coupland.
Identifying patients with suspected pancreatic cancer in primary care: Derivation and validation of an algorithm. The British Journal of General Practice.
2012;
62(594)
:
e38-e45
.
View Article PubMed Google Scholar -
N.
Howlader,
A. M.
Noone,
M.
Krapcho,
N.
Neyman,
R.
Aminou,
W.
Waldron,
S. F.
Altekruse.
Surveillance, Epidemiology, and End Results Program. Bethesda: National Cancer Institute.
2011
.
-
Q.-D.
Hu,
Q.
Zhang,
W.
Chen,
X.-L.
Bai,
T.-B.
Liang.
Human development index is associated with mortality-to-incidence ratios of gastrointestinal cancers. World Journal of Gastroenterology.
2013;
19(32)
:
5261-5270
.
View Article PubMed Google Scholar -
A.
Jemal,
F.
Bray,
M. M.
Center,
J.
Ferlay,
E.
Ward,
D.
Forman.
Global cancer statistics. CA: a Cancer Journal for Clinicians.
2011;
61(2)
:
69-90
.
View Article PubMed Google Scholar -
A.
Jemal,
M. M.
Center,
C.
DeSantis,
E. M.
Ward.
Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiology.
2010;
Biomarkers & Prevention
:
19(8)
.
View Article PubMed Google Scholar -
A.
Jemal,
R.
Siegel,
J.
Xu,
E.
Ward.
Cancer statistics, 2010. CA: a Cancer Journal for Clinicians.
2010;
60(5)
:
277-300
.
View Article PubMed Google Scholar -
A.
Jemal,
E. P.
Simard,
J.
Xu,
J.
Ma,
R. N.
Anderson.
Selected cancers with increasing mortality rates by educational attainment in 26 states in the United States, 1993-2007. Cancer Causes & Control.
2013;
24(3)
:
559-565
.
View Article PubMed Google Scholar -
Panos.
Kanavos.
The rising burden of cancer in the developing world. Annals of oncology.
2006;
17(suppl 8)
:
viii15-viii23
.
View Article Google Scholar -
M. G.
Keane,
L. J.
Horsfall,
G.
Rait,
S. P.
Pereira.
Sociodemographic trends in the incidence of pancreatic and biliary tract cancer in UK primary care. PLoS One.
2014;
9(9)
:
e108498
.
View Article PubMed Google Scholar -
N.
Keyghobadi,
H.
Rafiemanesh,
A.
Mohammadian-Hafshejani,
M.
Enayatrad,
H.
Salehiniya.
Epidemiology and trend of cancers in the province of Kerman: Southeast of Iran. Asian Pacific Journal of Cancer Prevention.
2015;
16(4)
:
1409-1413
.
View Article PubMed Google Scholar -
S. C.
Larsson,
J.
Permert,
N.
Håkansson,
I.
Näslund,
L.
Bergkvist,
A.
Wolk.
Overall obesity, abdominal adiposity, diabetes and cigarette smoking in relation to the risk of pancreatic cancer in two Swedish population-based cohorts. British Journal of Cancer.
2005;
93(11)
:
1310-1315
.
View Article PubMed Google Scholar -
A. B.
Lowenfels,
P.
Maisonneuve,
E. P.
DiMagno,
Y.
Elitsur,
L. K. Jr.
Gates,
J.
Perrault,
D. C.
Whitcomb,
the International Hereditary Pancreatitis Study Group..
Hereditary pancreatitis and the risk of pancreatic cancer. Journal of the National Cancer Institute.
1997;
89(6)
:
442-446
.
View Article PubMed Google Scholar -
A. B.
Lowenfels,
P.
Maisonneuve.
Epidemiology and risk factors for pancreatic cancer. Best Practice & Research. Clinical Gastroenterology.
2006;
20(2)
:
197-209
.
-
K.
Malik.
Human development report 2013. The rise of the south: Human progress in a diverse world. The Rise of the South: Human Progress in a Diverse World (March 15, 2013). UNDP-HDRO Human Development Reports.
2013;
2013
.
-
M.
Malvezzi,
P.
Bertuccio,
F.
Levi,
C.
La Vecchia,
E.
Negri.
European cancer mortality predictions for the year 2013. Annals of Oncology : Official Journal of the European Society for Medical Oncology.
2013;
24(3)
:
792-800
.
View Article PubMed Google Scholar -
C. D.
Mathers,
D. M.
Fat,
M.
Inoue,
C.
Rao,
A. D.
Lopez.
Counting the dead and what they died from: An assessment of the global status of cause of death data. Bulletin of the World Health Organization.
2005;
83(3)
:
171-177
.
PubMed Google Scholar -
D. S.
Michaud.
Epidemiology of pancreatic cancer. Minerva Chirurgica.
2004;
59(2)
:
99-111
.
PubMed Google Scholar -
M.
Mohammadian,
M.
Ghafari,
B.
Khosravi,
H.
Salehiniya,
M.
Aryaie,
F. A.
Bakeshei,
A.
Mohammadian-Hafshejani.
Variations in the Incidence and Mortality of Ovarian Cancer and Their Relationship with the Human Development Index in European Countries in 2012. Biomedical Research and Therapy.
2017;
4(08)
:
1541-1557
.
View Article Google Scholar -
M.
Mohammadian,
A.
Soroush,
A.
Mohammadian-Hafshejani,
F.
Towhidi,
F.
Hadadian,
H.
Salehiniya.
Incidence and Mortality of Liver Cancer and Their Relationship with Development in Asia. Asian Pacific Journal of Cancer Prevention.
2016;
17(4)
:
2041-2047
.
View Article PubMed Google Scholar -
T.
Muniraj,
P. A.
Jamidar,
H. R.
Aslanian.
Pancreatic cancer: A comprehensive review and update. Disease-a-Month.
2013;
59(11)
:
368-402
.
View Article PubMed Google Scholar -
J. E.
Muscat,
S. D.
Stellman,
D.
Hoffmann,
E. L.
Wynder.
Smoking and pancreatic cancer in men and women. Cancer Epidemiology, Biomarkers & Prevention.
1997;
6(1)
:
15-19
.
PubMed Google Scholar -
A.
Neesse,
P.
Michl,
K.K.
Frese,
C.
Feig,
N.
Cook,
M.A.
Jacobetz,
M.P.
Lolkema,
M.
Buchholz,
K.P.
Olive,
T.M. Tuveson
Gress.
Stromal biology and therapy in pancreatic cancer. Gut.
2011;
60(6)
:
861-868
.
-
J.P.
Neoptolemos,
D.D.
Stocken,
C.
Bassi,
P.
Ghaneh,
D.
Cunningham,
D.
Goldstein,
R.
Padbury,
M.J.
Moore,
S.
Gallinger,
C. Wente
Mariette.
Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: A randomized controlled trial. Journal of the American Medical Association.
2010;
304(10)
:
1073-1081
.
View Article PubMed Google Scholar -
J. P.
Neoptolemos,
J. A.
Dunn,
D. D.
Stocken,
J.
Almond,
K.
Link,
H.
Beger,
M. W.
Büchler,
the European Study Group for Pancreatic Cancer..
Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: A randomised controlled trial. Lancet.
2001;
358(9293)
:
1576-1585
.
View Article PubMed Google Scholar -
World Health.
Organization.
The world health report 2000: health systems: improving performance. World Health Organization.
2000
.
-
R.
Pakzad,
M.
Ghoncheh,
Z.
Pournamdar,
I.
Pakzad,
Z.
Momenimovahed,
H.
Salehiniya,
B. R.
Makhsosi.
Spatial Analysis of Skin Cancer Incidence in Iran. Asian Pacific Journal of Cancer Prevention.
2016;
17(sup3
:
S3)
.
View Article PubMed Google Scholar -
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of lung cancer and their relationship to development in Asia. Translational Lung Cancer Research.
2015a;
4(6)
:
763-774
.
View Article PubMed Google Scholar -
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of prostate cancer and its relationship with development in Asia. Prostate International.
2015b;
3(4)
:
135-140
.
View Article PubMed Google Scholar -
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Mohammadian,
I.
Pakzad,
S.
Safiri,
S.
Khazaei,
H.
Salehiniya.
Incidence and Mortality of Bladder Cancer and their Relationship with Development in Asia. Asian Pacific Journal of Cancer Prevention.
2015;
16(16)
:
7365-7374
.
View Article PubMed Google Scholar -
D. M.
Parkin,
F.
Bray,
J.
Ferlay,
P.
Pisani.
Global cancer statistics, 2002. CA: a Cancer Journal for Clinicians.
2005;
55(2)
:
74-108
.
View Article PubMed Google Scholar -
M. A.
Pourhoseingholi,
M.
Vahedi,
A. R.
Baghestani.
Burden of gastrointestinal cancer in Asia; an overview. Gastroenterology and Hepatology from Bed To Bench.
2014;
1(1)
.
PubMed Google Scholar -
H.
Rafiemanesh,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
Z.
Sepehri,
R.
Shamlou,
H.
Salehiniya,
B. R.
Makhsosi.
Incidence and mortality of colorectal cancer and relationships with the human development index across the world. Asian Pacific journal of cancer prevention. APJCP.
2016;
17(5)
:
2465-2473
.
PubMed Google Scholar -
M.
Ravallion.
Good and bad growth: The human development reports. World Development.
1997;
25(5)
:
631-638
.
View Article Google Scholar -
Saeid
Razi.
The incidence and mortality of ovarian cancer and their relationship with the Human Development Index in Asia. ecancermedicalscience.
2016;
10
.
-
J. K.
Ryu,
S. M.
Hong,
C. A.
Karikari,
R. H.
Hruban,
M. G.
Goggins,
A.
Maitra.
Aberrant MicroRNA-155 expression is an early event in the multistep progression of pancreatic adenocarcinoma. Pancreatology.
2010;
10(1)
:
66-73
.
View Article PubMed Google Scholar -
A. R.
Sasson,
J. P.
Hoffman,
E. A.
Ross,
S. A.
Kagan,
J. F.
Pingpank,
B. L.
Eisenberg.
En bloc resection for locally advanced cancer of the pancreas: Is it worthwhile?. Journal of Gastrointestinal Surgery.
2002;
6(2)
:
147-157
.
-
G. G.
Schwartz,
I. M.
Reis.
Is cadmium a cause of human pancreatic cancer?. Cancer Epidemiology, Biomarkers & Prevention.
2000;
9(2)
:
139-145
.
PubMed Google Scholar -
M.
Shuja,
S. I.
Farsani,
H.
Salehiniya,
S.
Khazaei,
M.
Mohammadian,
M.
Aryaie,
A.
Mohammadian-Hafshejani.
Assessment the association between liver cancer incidence and mortality rate with human development index in the European countries in 2012. Biomedical Research and Therapy.
2017;
4(03)
:
1185-1197
.
View Article Google Scholar -
R.
Siegel,
D.
Naishadham,
A.
Jemal.
Cancer statistics, 2012. CA: a Cancer Journal for Clinicians.
2012;
62(1)
:
10-29
.
View Article PubMed Google Scholar -
D. T.
Silverman,
J. A.
Dunn,
R. N.
Hoover,
M.
Schiffman,
K. D.
Lillemoe,
J. B.
Schoenberg.
Cigarette smoking and pancreas cancer: A case-control study based on direct interviews. Journal of the National Cancer Institute.
1994;
86(20)
:
1510-1516
.
View Article PubMed Google Scholar -
B. D.
Smith,
G. L.
Smith,
A.
Hurria,
G. N.
Hortobagyi,
T. A.
Buchholz.
Future of cancer incidence in the United States: Burdens upon an aging, changing nation. Journal of Clinical Oncology.
2009;
27(17)
:
2758-2765
.
View Article PubMed Google Scholar -
American Cancer.
Society.
Cancer facts and figures 2013. American Cancer Society Atlanta.
2013
.
-
S.
Stapley,
T. J.
Peters,
R. D.
Neal,
P. W.
Rose,
F. M.
Walter,
W.
Hamilton.
The risk of pancreatic cancer in symptomatic patients in primary care: A large case-control study using electronic records. British Journal of Cancer.
2012;
106(12)
:
1940-1944
.
View Article PubMed Google Scholar -
F.
Stats.
An interactive tool for access to SEER cancer statistics. Surveillance Research Program. National Cancer Institute.
2012
.
-
A.
Tiyuri,
A.
Mohammadian-Hafshejani,
E.
Iziy,
H. S.
Gandomani,
H.
Salehiniya.
The incidence and mortality of lip and oral cavity cancer and its relationship to the 2012 Human Development Index of Asia. Biomedical Research and Therapy.
2017;
4(02)
:
1147-1165
.
View Article Google Scholar -
A. T.
Toriola,
R.
Stolzenberg-Solomon,
L.
Dalidowitz,
D.
Linehan,
G.
Colditz.
Diabetes and pancreatic cancer survival: A prospective cohort-based study. British Journal of Cancer.
2014;
111(1)
:
181-185
.
View Article PubMed Google Scholar -
S.
Valean,
M.
Acalovschi,
M.
Diculescu,
M.
Manuc,
A.
Goldis,
C.
Sfarti,
A.
Trifan.
Mortality in Digestive Cancers, 2012: International Data and Data from Romania. Journal of Gastrointestinal and Liver Diseases; JGLD.
2015;
24(4)
:
507-514
.
PubMed Google Scholar -
L.
Wang,
G.-H.
Yang,
X.-H.
Lu,
Z.-J.
Huang,
H.
Li.
Pancreatic cancer mortality in China (1991-2000). WJG.
2003;
9(8)
:
1819-1823
.
View Article PubMed Google Scholar -
E.
Ward,
A.
Jemal,
V.
Cokkinides,
G. K.
Singh,
C.
Cardinez,
A.
Ghafoor,
M.
Thun.
Cancer disparities by race/ethnicity and socioeconomic status. CA: a Cancer Journal for Clinicians.
2004;
54(2)
:
78-93
.
View Article PubMed Google Scholar
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 02 (2018)
Page No.: 1986-1999
Published on: 2018-02-26
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 5533 times
- Download PDF downloaded - 1371 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}