

Copyrights: Mahdi Mohammadian, Khadijah Allah Bakeshei, Hamid Salehiniya, Fatemeh Allah Bakeshei, Abdollah Mohammadian-Hafshejani, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Breast cancer (BC) is the most common cancer malignancy and the important reason for cancer-related mortality in females. The aim of this study was to evaluate the geographical distribution of occurrence and mortality of BC and their association with Human Development Index (HDI) in Europe in 2012.
Methods: This was an ecologic study to evaluate the relation between Age-Standardized Incidence Rate (ASIR) and Age Standardized Mortality Rate (ASMR) of BC with HDI, using data of GLOBOCAN project and the HDI report. Using SPSS18 statistical analysis software the data of the study was analyzed; the significance level of the tests was considered as P 0.05.
Results: The highest ASIR of BC was observed in Belgium, Denmark, the Netherlands and the highest ASMR was found in the FYR Macedonia, Serbia, Belgium, respectively. A positive correlation was found between the ASIR of BC and HDI (r= 0.611, p≤ 0.001), life expectancy in birth (r= 0.706, p≤0.001), average education years (r=0.038, p=0.815) and gross national income per capita (r= 0.719, p≤0.001). Moreover, there was negative correlation between the ASMR of BC and HDI (r= 0.464, p= 0.003), life expectancy at birth (r= 0.416, p=0.008), average education years (r= 0.277, p= 0.083) and gross national income per capita (r= 0.255, p= 0.112). Moreover, it is expected that the number of incidence and mortality from BC is increased within 2012-2035 in European countries.
Conclusion: There is a positive correlation between the ASIR of BC and HDI. Moreover, there is a negative correlation between ASMR of BC with HDI. Therefore, the results of this study indicate the importance of using HDI as factors affecting the ASIR and ASMR of BC.
Background
Breast cancer (BC) is the most common cancer malignancy and the important reason for cancer related-mortality in females [1]. Distribution of new cases of BC was very various in the world, hence, the minimum incidence observed in Asia with Age-Standardized Incidence Rate (ASIR) was 29.1 per 100,000 women and the maximum in Northern America with ASIR was 91.6 per 100,000 women [2][3]. In 2012, in European countries, there were an estimated 463,800 cases of new BC and 131,200 cases of BC-related deaths. In the United States, almost 5% of patients with BC are identified with metastatic disease at first presentation [4]. Moreover, a recent study showed that about 10% of patients diagnosed with early-stage of BC developed metastatic illness within an average of 5.7 years follow-up [5].
However, in recent years deaths from BC are declining in Australia, North America, and Western and most Nordic European countries [6]–[8]. After more than 20 years of severe mammography screening programs in some of these countries, it is still difficult to determine the amount of the detected decrease in mortality of BC attributed to prior diagnosis or to enhance the management programs. This trouble arises from the limited capacity of observational studies to indicate the effects of primary diagnosis, treatment, and output of healthcare systems on the mortality [9].
Early detection of cancer is vital to decrease the mortality rate and to increase the survival rate of disease [10]. The survival rate of BC is different in the world based on the regional location and socio-economic status [11], hence, in the low-income countries it was less than 40%, and in the high-income countries, it was more than 80%. The low survival of BC in developing countries was related to deficiency of diagnostic and treatment programs [12].
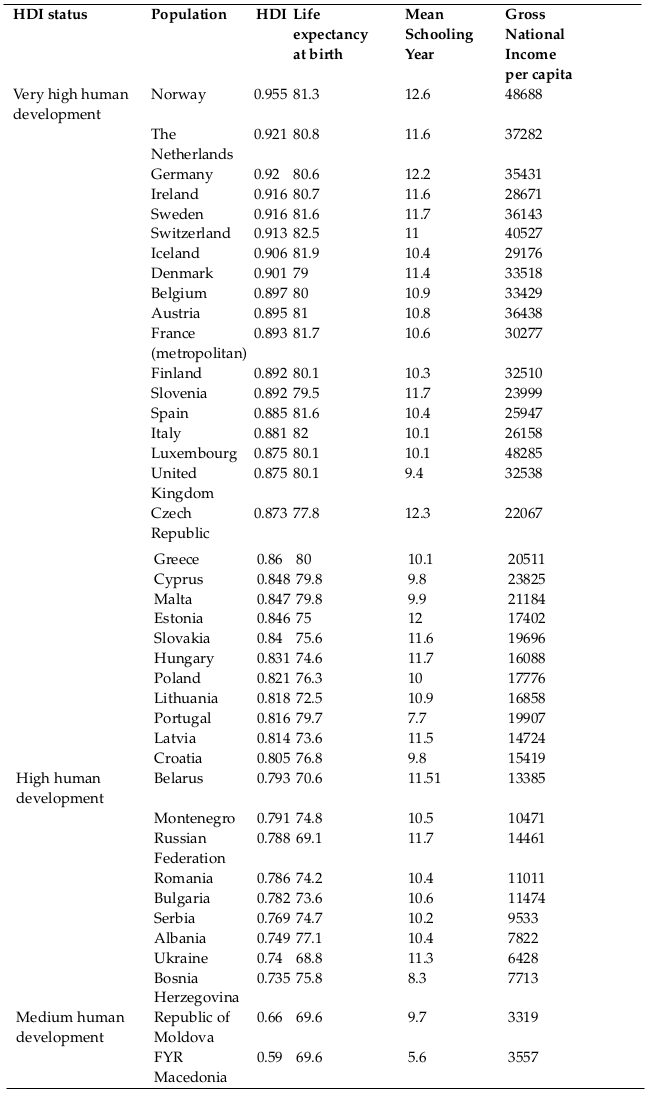
Socioeconomic factors are related to cancer incidence and mortality through complex and changeable pathways. Human Development Index (HDI) is one of the most significant known indicators of socioeconomic factors. The HDI was recommended by UNDP as an indicator for evaluating and comparing the nations in three human aspects including life expectancy at birth, average schooling years and gross national income per capita. Based on HDI, countries are allocated into four classes: Countries with very high HDI (HDI≥ 0.9), countries with high HDI (0.9>HDI≥0.8), countries with Medium HDI (0.8>HDI>0.5), and countries with low HDI (HDI≤0.5) [13]. In the present study, HDI was used as an indicator of socioeconomic factors [14]. In a study conducted in Asia, a positive relation was found between ASIR of BC and HDI. However, this relationship between ASMR and HDI wasn’t significant [15] . Similarly in other studies the association between incidence and mortality of other cancers and HDI were examined [16]–[21]. In most of these studies, a significant association was observed between ASIR, ASMR, and HDI. Therefore, in this study, we investigate the geographical distribution and predict the trend of incidence and mortality of BC and their association with Human Development Index (HDI) in Europe, using data of GLOBOCAN project and the human development index report.
Methods
This ecologic study conducted in European countries for appraisement of the correlation among the Age-Standardized Incidence Rate (ASIR) and Age Standardized Mortality Rate (ASMR), and Human development index (HDI) and its components including the average education years, life expectancy at birth, and gross national income per capita. Information on the ASIR for each of European countries for 2012 were acquired from the GLOBOCAN project of World Health Organization (WHO), which is accessible from (http://globocan.iarc.fr/Default.aspx), and statistics on the HDI was gained from the Global report of Human Development index in 2013 [13], that counting definite evidence about the HDI and its components for each of country in the word for 2012.
The method for estimation of the ASIR and ASMR in the GLOBOCAN project
In the GLOBOCAN project, the estimation methods of ASIR and ASMR are particular for each country; therefore, quality of the estimate for each country depends on the quality and the extent of data available for each country. Hence, since methods in every country are specific, determining an overall quality score for the ASIR and ASMR estimations is almost impossible. A detailed description of the material and methods utilized in this scheme provided in previous reports [2].
Human development index (HDI)
In the current study, Human development index (HDI) was used as an indicator of socioeconomic factors [14]. HDI is a complex measure of indicators along with three dimensions including health, education, and standard of living. The HDI is the geometric average of normalized indices for every three dimensions. The health dimension is measured with life expectancy at birth; the education dimension is evaluated by average schooling years for adults and expected schooling years for children, the standard of living dimension is evaluated by gross national income per capita. The scores for HDI dimension indicator are then combined into a complex index using the geometric average [13].
Statistical analysis
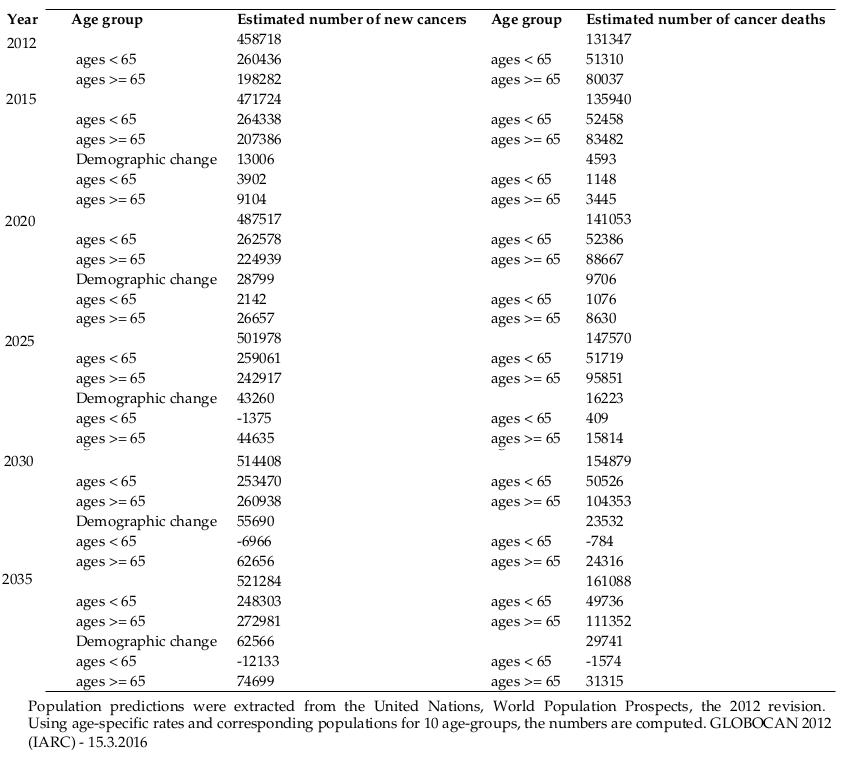
In the present study, the correlation bivariate method was used to evaluate the correlation between ASIR and ASMR with HDI, and its components including; average education years, life expectancy at birth, and gross national income per capita. In GLOBOCAN project, the estimated number of new cases and deaths of BC in a region in 2015, 2020, 2025, 2030 and 2035 is calculated by multiplying the age-specific rates estimated for 2012, by the corresponding expected population for 2015, 2020, 2025, 2030 and 2035. In this study, the statistical significance was considered as P < 0.05. Whole stated P-values are two-sided. The SPSS (Version 18.0, SPSS Inc.) was used to analyze the study data.
Results
Overall in 2012, European countries have recorded 458718 cases of BC, in which 5 countries with the highest number of BC are as the following: Germany with 71623 cases, Russian Federation with 57502 cases, the United Kingdom with 52399 cases, Italy with 50658 cases and France (metropolitan) with 48763 cases, that these five countries totally allocated 280945 cases (61.24%) of BC to themselves.
Furthermore, in European countries in 2012, 131347 cases of deaths occurred caused by BC, among which the five countries with the highest death number are as the following; Russian Federation with 24544 cases, Germany with 16828 cases, Italy with 12796 cases, France (metropolitan) with 11933 cases and the United Kingdom with 11679 cases. These five countries allocated 77780 cases (59.21%) of BC mortality to themselves.
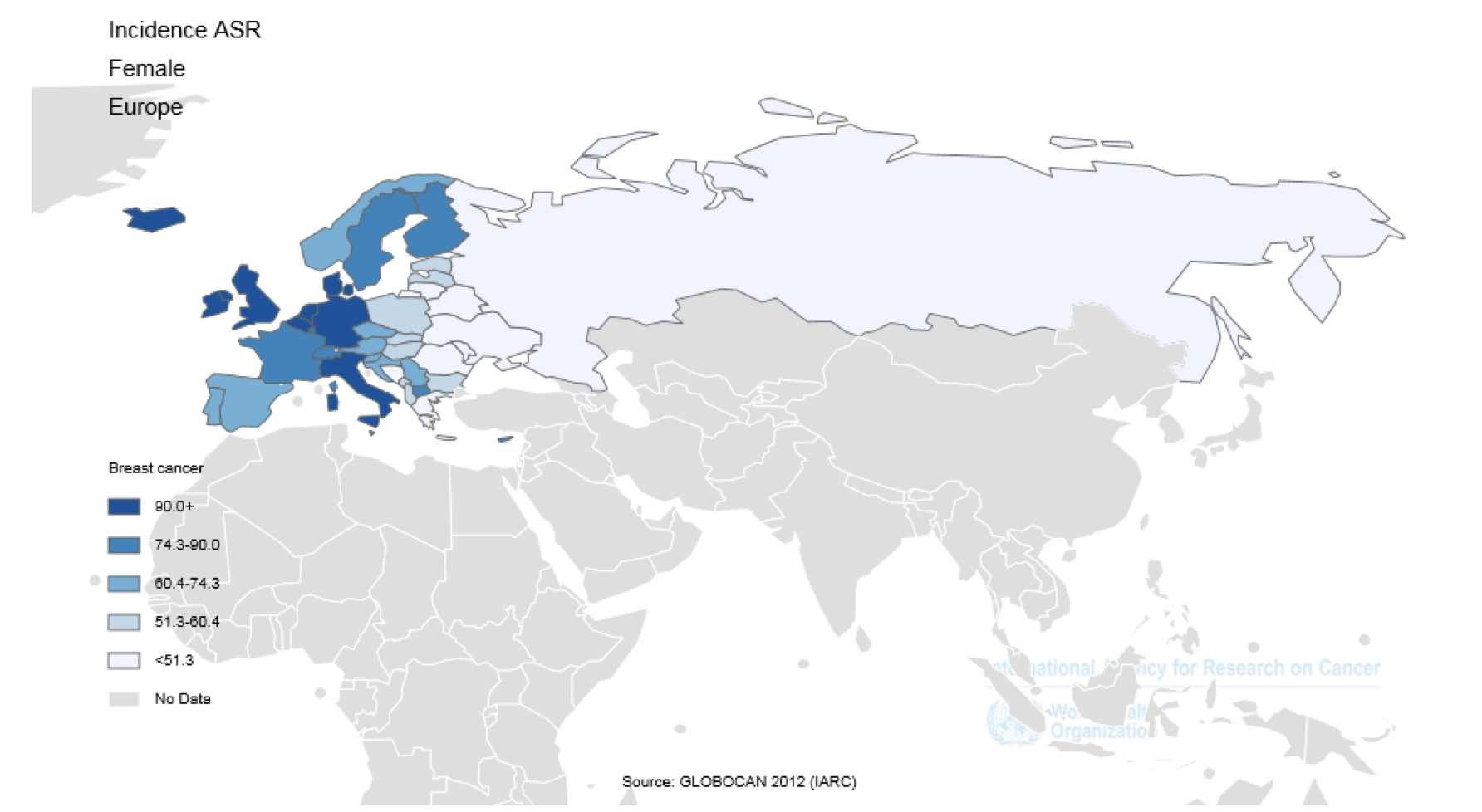
The five countries that have the highest ASIR of the BC per hundred thousand people are as the following; Belgium with 111.9, Denmark with 105, the Netherlands with 99, Iceland with 96.3, and the United Kingdom with 95. In contrast, five countries with the lowest ASIR of the BC were Bosnia Herzegovina with 37.4, the Republic of Moldova with 38.7, Ukraine with 41.3, Greece with 43.9, and Russian Federation with 45.6. The number, crude and standardized incidence rates of the BC in European countries based on sex are presented in Table 1 . The countries with the highest and the lowest ASIR in both sexes are observed in Table 1 and Figure 1 and Figure 3 .
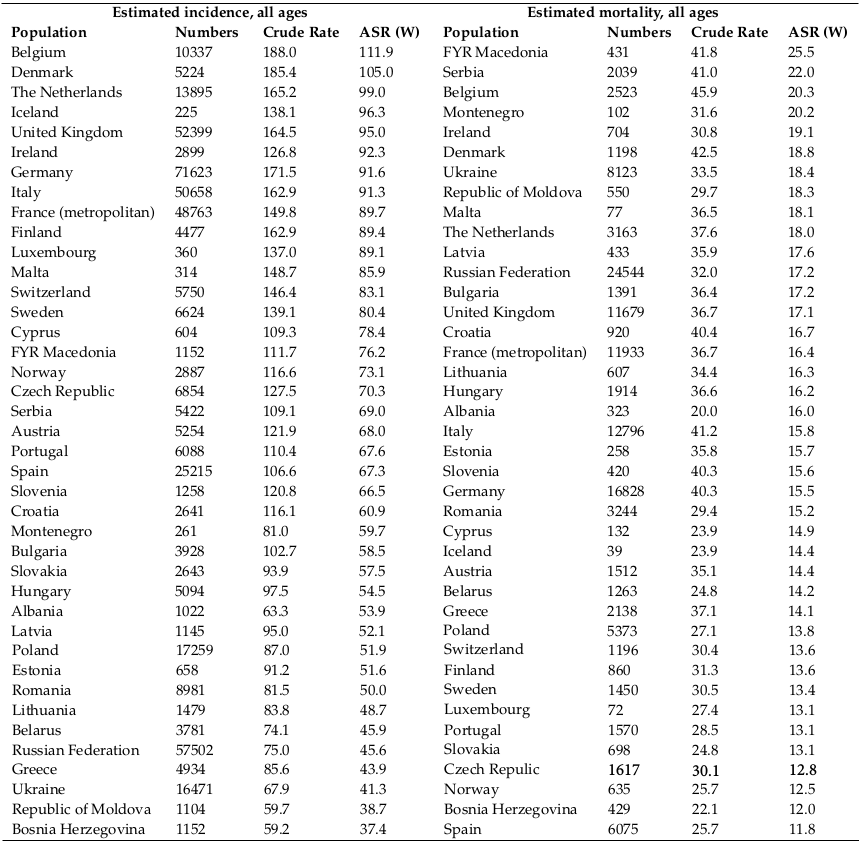
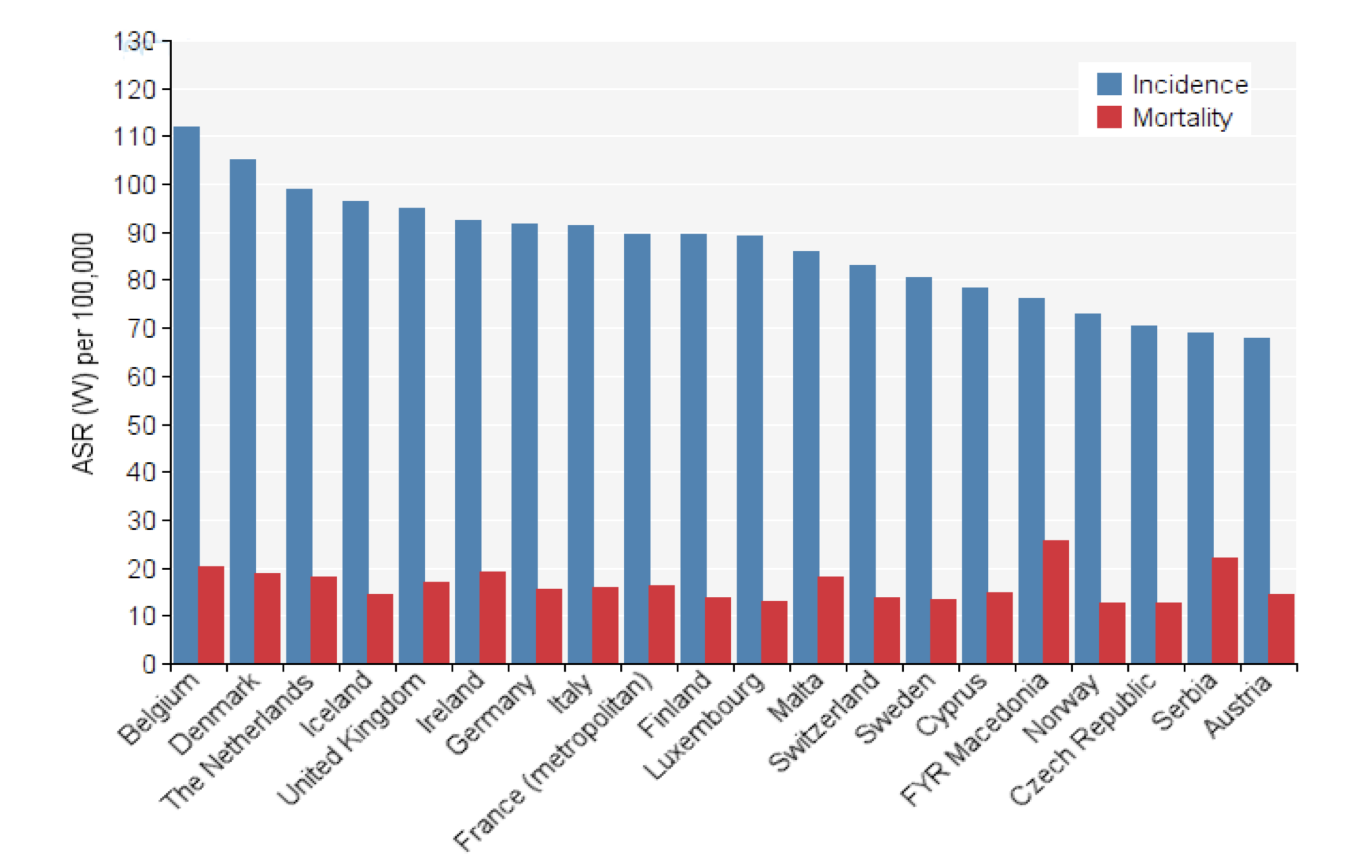
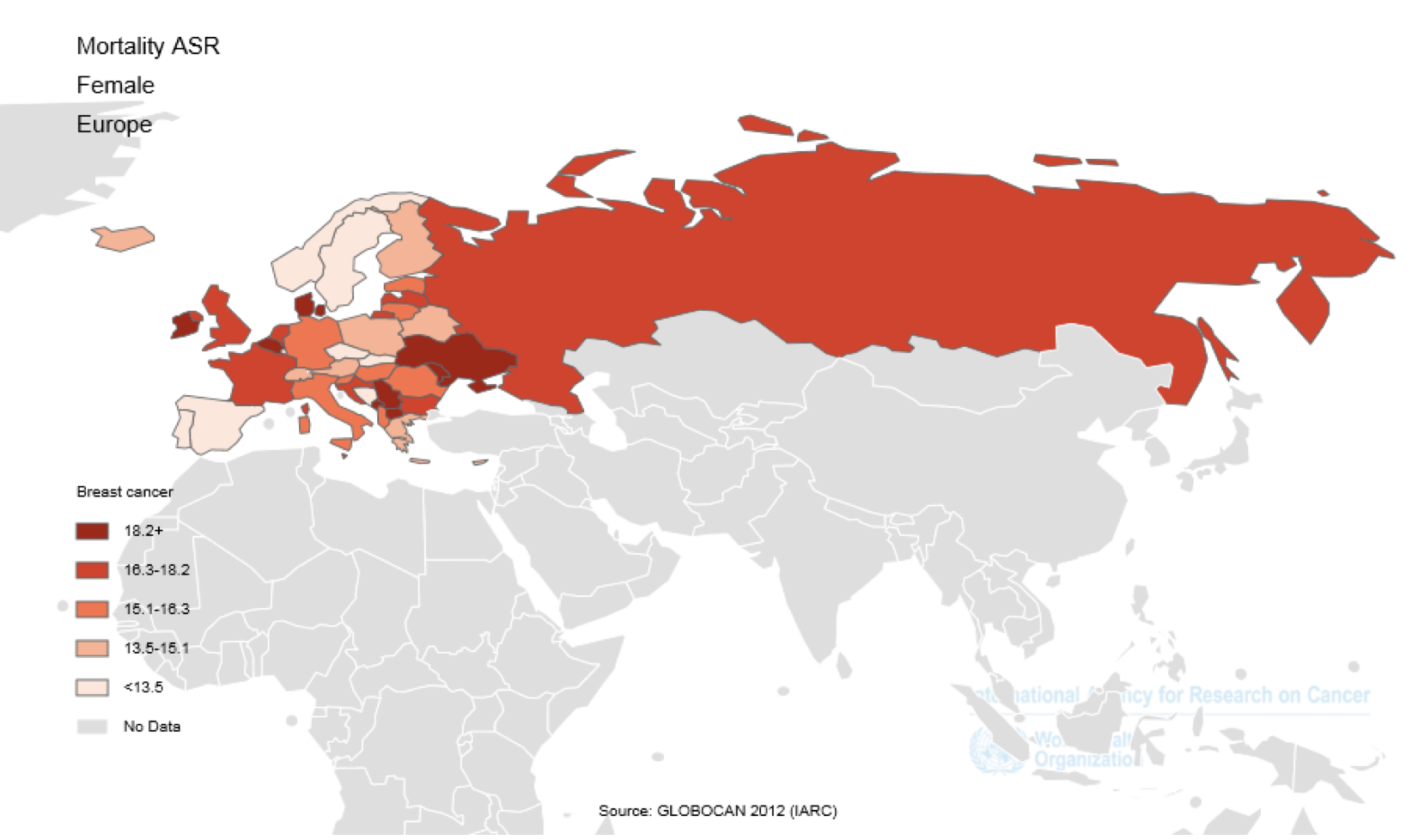
The five countries with the highest ASMR from BC per hundred thousand people are as the following: FYR Macedonia with 25.5, Serbia with 22, Belgium with 20.3, Montenegro with 20.2 and Ireland with 19.1. In contrast, the five countries with the lowest ASMR from BC are as the following: Spain with 11.8, Bosnia Herzegovina with 12, Norway with 12.5, the Czech Republic with 12.8 and Slovakia with 13.1 Table 1 Figure 2 and Figure 3 .
In 2012, some 458718 new cases of BC were observed in the European countries, that 260436 cases (56.77%) are in the age group under 65 years old and 198282 cases (43.23%) are in the age group of 65 years old and higher. According to the forecasts, it is expected that in the years 2015, 2020, 2025, 2030 and 2035 the number of new cases, would be 471724, 487517, 501978, 514408 and 521284, respectively, indicating that over these years the number of new BC cases,
increased to 13006, 28799, 43260, 55690 and 62566 cases, respectively, compared to 2012. In fact, over these years the number of new cases is increased to 02.83%, 06.27%, 09.43%, 12.14% and 13.63%, respectively. Although it is predicted that the number of new cases increases within 2012 and 2035, it is predictable that this increase will be more in the age group of 65 years and higher, nonetheless in the age group under 65 years the number of cases will be reduced.
Furthermore, in 2012, about 131347 cases of death were observed in European countries, among which 51310 cases (39.06%) are in the age group under 65 years, and 80037 cases (60.93%) are in the age group of 65 years and higher. According to the predictions, it is expected that in the years 2015, 2020, 2025, 2030 and 2035 the number of death cases, would be 135940, 141053, 147570, 154879 and 161088 cases, respectively, indicating that over these years the number of deaths from the disease increased to 4593, 9706, 16223, 23532 and 29741 cases, compared to 2012. In fact, the
number of death increases to 03.49%, 07.38%, 12.35%, 17.91% and 22.64%, respectively. Although it is expected that the number of deaths from BC to increase within 2012 and 2035, it is predictable that this increase will be observed in the age group of 65 years and higher and the number of death from BC will reduce in the age group under 65 years Table 2 .
In Table 3 , the respective value of the HDI and its components were shown for each European country that is arranged based on the HDI index. Thus in Europe, countries are classified regarding HDI as the following, so that 29 countries classified as a very high category, nine countries as a high category and two countries are classified as the medium category.
ASIR and HDI
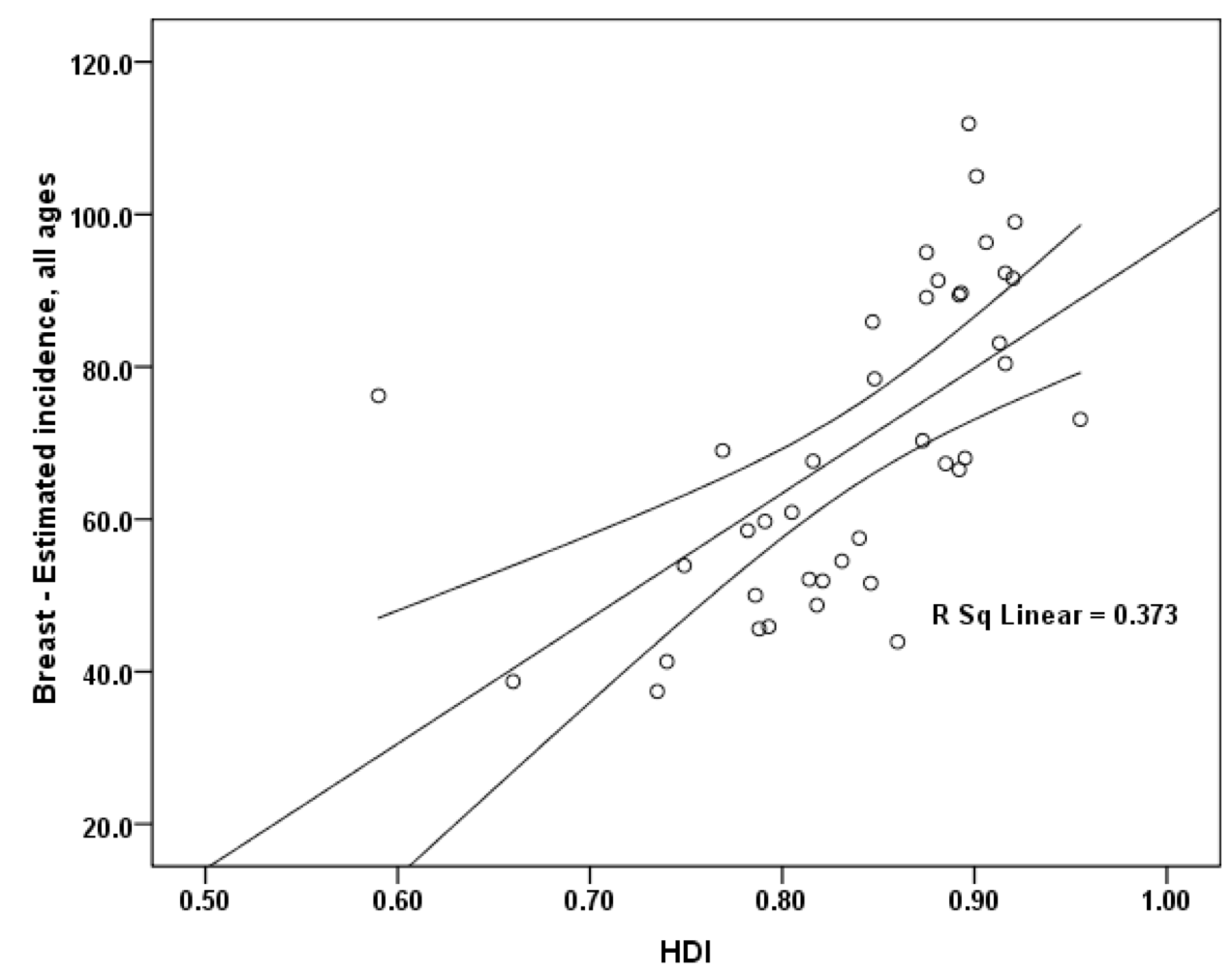
A positive statically significant correlation equal to 0.611 was found between the ASIR of BC and HDI (p≤ 0.001). Moreover, a correlation was observed between the components of the HDI and ASIR. So that the ASIR with life expectancy in birth had a positive correlation of 0.706 (p≤ 0.001), positive correlation of 0.038 with the average education years (p=0.815) and it had a positive correlation of 0.719 (p≤0.001) with gross national income per capita Figure 4 .
ASMR and HDI
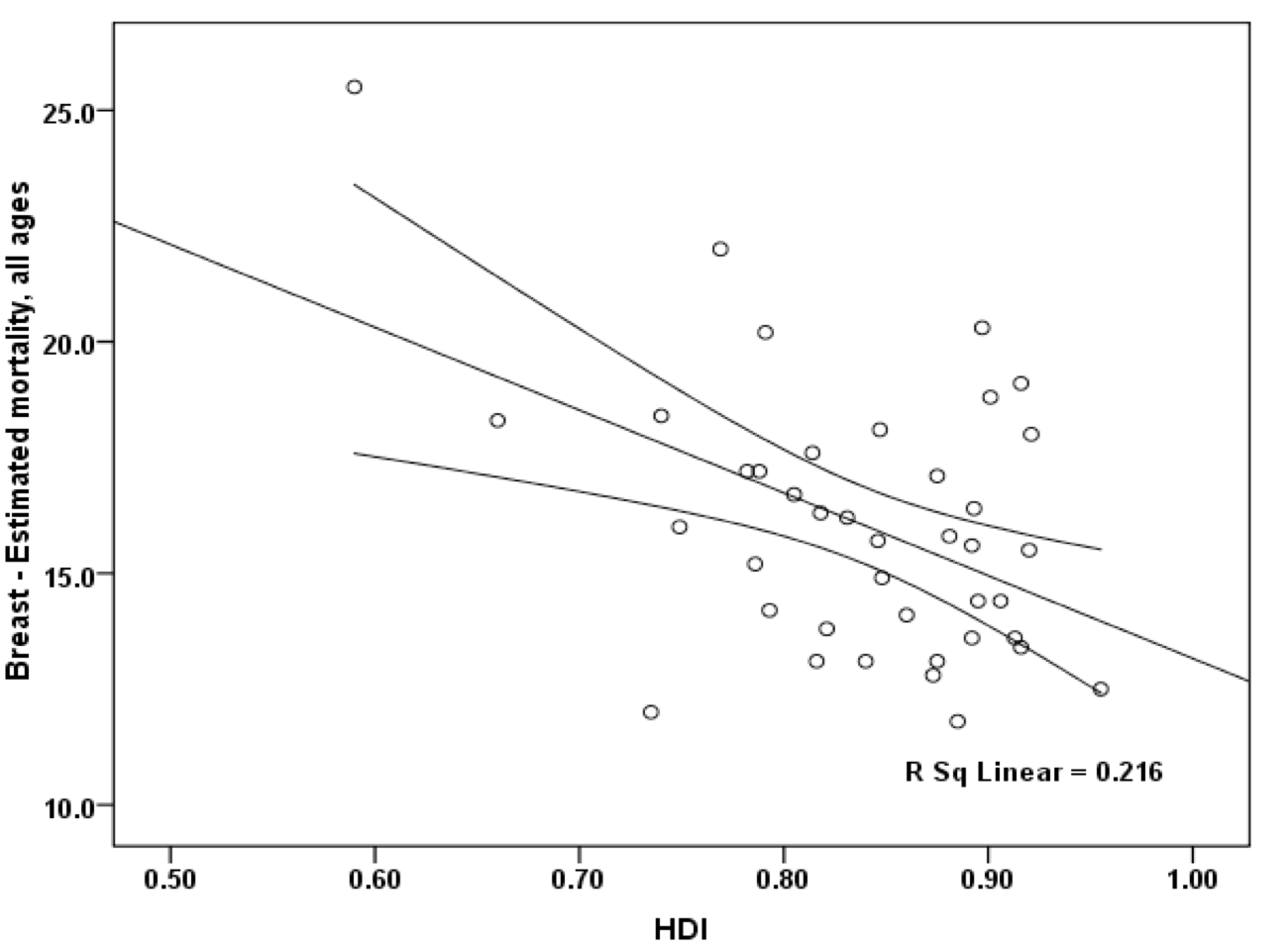
Furthermore, between the ASMR of BC and HDI, a negative correlation of 0.464 was observed, that this association was statistically significant (p=0.003). Moreover, a correlation was observed between the components of the HDI and ASMR, so that the ASMR with life expectancy at birth had a negative correlation of 0.416 (p=0.008), a negative correlation of 0.277 (p=0.083) with the average education years and it had negative correlation equal to 0.255 (p=0.112) with gross national income per capita Figure 5 .
Discussion
In the present study geographical distribution of incidence and mortality of BC and their association with the HDI in European countries in 2012 were examined. Among European countries the highest ASIR of the BC were observed in Belgium, Denmark, the Netherlands, Iceland, and the United Kingdom, respectively. In addition, the highest ASMR from BC was observed in FYR Macedonia, Serbia, Belgium, Montenegro, and Ireland, respectively. We found that there is a positive correlation between ASIR of BC and HDI and their component. Moreover, there is a negative correlation between the ASMR of BC and HDI and its components. Moreover, it is anticipated that within 2012 and 2035, the number of new cases and the number of deaths caused by BC in the age group of 60 and higher has been increased and it has been declined in the age group under 65 years.
Our results showed that the occurrence of BC in Europe was related to HDI and its components [13]. Among European countries¸Belgium with 111.9 per 100,000, Denmark with 105 per 100,000, the Netherlands with 99 per 100,000, Iceland with 96.3 per 100,000, and the United Kingdom with 95 per 100,000 had the highest ASIR of BC. All these countries were in the very high HDI categories. In contrast, in countries such as Bosnia Herzegovina with 37.4 per 100,000, the Republic of Moldova with 38.7 per 100,000, Ukraine with 41.3 per 100,000, Greece with 43.9 per 100,000, and Russian Federation with 45.6 per 100,000 the lowest ASIR was observed. However, among these countries, only Greece was in the very high HDI category.
Life expectancy at birth is one of the HDI dimensions [13]. It is directly associated with the occurrence of cancer as well as BC. The risk of chronic diseases such as cancer is increased along with the country development, the removal of competing causes of death, and increasing of life expectancy. This can be associated with increasing the exposure time to risk factors in individuals [22]. In the study conducted in Asian countries regarding BC and HDI, a significant correlation was observed between the ASIR of BC and life expectancy at birth [15].
The second component of HDI is average schooling years. Studies indicated the existence of a positive relationship between average schooling years and individuals’ behavior [23]. Increasing the knowledge, education, and employment, women probably perform breast self-examination, thus, looking for diagnostic methods significantly is increased [24]. Hence, in these countries, BC is diagnosed much earlier compared to the countries with lower knowledge levels. In our study, no significant relationship was found between average schooling years and ASIR and ASMR of BC. However, in the study of Ghoncheh et al., in Asia, a significant correlation was observed between ASIR of BC and average schooling years, but the relation between average schooling years and ASMR wasn’t significant [15].
The third HDI component is gross national income per capita. According to the report of the World Health Organization (WHO), increasing income and improving the living standards in developing countries led to the intensification in the incidence of BC [25]. This may be caused by the longer life, higher exposure to risk factors, eating more fatty foods and obesity, and lower pregnancy rates [14]. With the increasing development, the incidence of cancers such as BC is increased, and the cancers associated with infectious agents are reduced [14]. Similar to this study, in the study of Ghoncheh et al., in Asia, a significant correlation was observed between ASIR of BC and gross national income per capita [15]. In high-income countries, the advantage of better diagnostic methods significantly is better compared to the other countries [11]. In fact, diagnosis of cancer in high-income countries is conducted better than low-income countries. In other words, some of BC cases in low-income countries weren’t diagnosis and report properly.
Among European countries, the five countries with the lowest ASMR of BC are as the following: Spain, Bosnia Herzegovina, Norway, the Czech Republic and Slovakia, respectively. In five countries with the lowest ASMR from BC except for Bosnia Herzegovina, all other countries were in very high human development category. There was a significant negative linear relationship between ASMR and HDI of BC. In the study of Gonzaga et al., in Brazil, there was a significant relationship between HDI and cancer mortality [26]. However, in the study of Ghoncheh et al., in Asia, there was not a significant correlation between the ASMR of BC and HDI and its components [15].
The present study involves some advantages. The first advantage is that the data include perfect integrity since we studied all European countries. The second advantage is the introduction of HDI and its components as risk factors for incidence and mortality of BC in European countries which can help the risk factors determination of this disease. The third advantage is the novelty of findings since we couldn’t find a study indicating the relationship between the ASIR and ASMR of BC with HDI and its components in European countries.
However, this study includes some limitations. The first limitation is that this study was an ecological study and its results can be interpreted solitary at the population level. Therefore, the ascription of the consequences of this study to individual levels leads to happening the ecological fallacy. The second limitation of this study was different in cancer data collection, diagnosis, and care method among countries entered in the study. Therefore, it is presented that analogous studies in other parts of the world must be conducted so that the association between the ASIR and ASMR of BC and HDI in these areas can be inspected.
Conclusion
According to the results of this study, it is expected that the number of incidence and mortality from BC is increased within 2012 and 2035 in European countries. There are positive correlations between the ASIR of BC with HDI. Moreover, there is a negative correlation between ASMR of BC with HDI. Therefore, the statistics from this study represent the importance of using HDI as factors affecting the ASIR and ASMR of BC.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
List of Abbreviations
ASIR: Age-Standardized Mortality Rate; ASMR: Age-Standardized Incidence Rate; BC: Breast Cancer; HDI: Human Development Index
Competing interests
The authors declare that no competing interests exist.
Authors’ contributions
All authors contributed to the design of the research. MM, KAB, and HS collected the data. HS, FAB, and AMH conducted analysis and interpretation of data. All authors drafted the first version. MM, AMH edited the first draft. All authors reviewed and commented on the final draft.
References
-
A
Jemal,
F
Bray,
MM
Center,
J
Ferlay,
E
Ward,
D
Forman.
Global cancer statistics. CA: a Cancer Journal for Clinicians.
2011;
61
:
69-90
.
View Article PubMed Google Scholar -
JS
Ferlay,
M
Ervik,
R
Dikshit.
GLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC cancer base No. 11. 2013
.
-
I
Soerjomataram,
DRESMCFJ
Ervik M.
GLOBOCAN 2012 v1. 0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11. 2013. International Agency for Research on Cancer Web site. 2014
.
-
J
Ferlay,
E
Steliarova-Foucher,
J
Lortet-Tieulent,
S
Rosso,
JW
Coebergh,
H
Comber.
Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. European Journal of Cancer.
2013;
(Oxford
:
England) 49
.
View Article PubMed Google Scholar -
E
Colzani,
AL
Johansson,
A
Liljegren,
T
Foukakis,
M
Clements,
J
Adolfsson.
Time- dependent risk of developing distant metastasis in breast cancer patients according to treatment, age and tumour characteristics. British Journal of Cancer.
2014;
110
:
1378-84
.
View Article PubMed PMC Google Scholar -
P
Autier,
M
Boniol,
CL
Vecchia,
L
Vatten,
A
Gavin,
C
Héry.
Disparities in breast cancer mortality trends between 30 European countries: retrospective trend analysis of WHO mortality database. BMJ (Clinical Research Ed.).
2010;
341
:
c3620
.
-
C
Héry,
J
Ferlay,
M
Boniol,
P
Autier.
Quantification of changes in breast cancer incidence and mortality since 1990 in 35 countries with Caucasian-majority populations. Annals of Oncology : Official Journal of the European Society for Medical Oncology.
2008;
19
:
1187-94
.
View Article PubMed Google Scholar -
A
Jemal,
R
Siegel,
J
Xu,
E
Ward.
Cancer statistics, 2010. CA: a Cancer Journal for Clinicians.
2010;
60
:
277-300
.
View Article PubMed Google Scholar -
DA
Berry,
KA
Cronin,
SK
Plevritis,
DG
Fryback,
L
Clarke,
M
Zelen,
I
Cancer,
CSM
Network.
Effect of screening and adjuvant therapy on mortality from breast cancer. The New England Journal of Medicine.
2005;
353
:
1784-92
.
View Article PubMed Google Scholar -
M
Rahimzadeh,
AR
Baghestani,
MR
Gohari,
MA
Pourhoseingholi.
Estimation of the cure rate in Iranian breast cancer patients. Asian Pacific Journal of Cancer Prevention.
2014;
15
:
4839-42
.
View Article PubMed Google Scholar -
H
Abbastabar,
P
Hamidifard,
A
Roustazadeh,
SH
Mousavi,
S
Mohseni,
M
Sepandi.
Relationships between breast cancer and common non- communicable disease risk factors: an ecological study. Asian Pacific Journal of Cancer Prevention.
2013;
14
:
5123-5
.
View Article PubMed Google Scholar -
DR
Youlden,
SM
Cramb,
NA
Dunn,
JM
Muller,
CM
Pyke,
PD
Baade.
The descriptive epidemiology of female breast cancer: an international comparison of screening, incidence, survival and mortality. Cancer Epidemiology.
2012;
36
:
237-48
.
View Article PubMed Google Scholar -
K
Malik.
Human development report 2013. The rise of the South: Human progress in a diverse world. The Rise of the South: Human Progress in a Diverse World (March 15, 2013).
2013
.
-
F
Bray,
A
Jemal,
N
Grey,
J
Ferlay,
D
Forman.
Global cancer transitions according to the Human Development Index (2008-2030): a population-based study. The Lancet. Oncology.
2012;
13
:
790-801
.
View Article Google Scholar -
M
Ghoncheh,
A
Mohammadian-Hafshejani,
H
Salehiniya.
Incidence and mortality of breast cancer and their relationship to development in Asia. Asian Pacific Journal of Cancer Prevention.
2015;
16
:
6081-7
.
View Article PubMed Google Scholar -
S
Hassanipour-Azgomi,
A
Mohammadian-Hafshejani,
M
Ghoncheh,
F
Towhidi,
S
Jamehshorani,
H
Salehiniya.
Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate International.
2016;
4
:
118-24
.
View Article PubMed PMC Google Scholar -
R
Pakzad,
A
Mohammadian-Hafshejani,
M
Ghoncheh,
I
Pakzad,
H.
Salehiniya.
The incidence and mortality of lung cancer and their relationship to development in Asia. Translational Lung Cancer Research.
2015a;
4
:
763-74
.
PubMed PMC Google Scholar -
R
Pakzad,
A
Mohammadian-Hafshejani,
M
Ghoncheh,
I
Pakzad,
H.
Salehiniya.
The incidence and mortality of prostate cancer and its relationship with development in Asia. Prostate International.
2015b;
3
:
135-40
.
View Article PubMed PMC Google Scholar -
H
Rafiemanesh,
A
Mohammadian-Hafshejani,
M
Ghoncheh,
Z
Sepehri,
R
Shamlou,
H
Salehiniya.
Incidence and Mortality of Colorectal Cancer and Relationships with the Human Development Index across the World. 2016;
17
:
2465-73
.
-
R
Pakzad,
A
Mohammadian-Hafshejani,
B
Khosravi,
S
Soltani,
I
Pakzad,
M
Mohammadian.
The incidence and mortality of esophageal cancer and their relationship to development in Asia. Annals of Translational Medicine.
2016;
4
:
29
.
PubMed PMC Google Scholar -
R
Pakzad,
A
Mohammadian-Hafshejani,
M
Mohammadian,
I
Pakzad,
S
Safiri,
S
Khazaei.
Incidence and Mortality of Bladder Cancer and their Relationship with Development in Asia. Asian Pacific Journal of Cancer Prevention.
2015;
16
:
7365-74
.
View Article PubMed Google Scholar -
J
Ferlay,
C
Héry,
P
Autier,
R
Sankaranarayanan.
Global burden of breast cancer Breast cancer epidemiology. 2010
.
-
MX
Liu,
J
Li,
YL
Geng,
YC
Wang,
J
Li,
YJ
Chen.
Correlation study of knowledge and behavior regarding breast care among female undergraduate students in China. Asian Pacific Journal of Cancer Prevention.
2014;
15
:
10943-7
.
View Article PubMed Google Scholar -
E
Ceber,
G
Mermer,
F
Okcin,
D
Sari,
M
Demireloz,
A
Eksioglu.
Breast cancer risk and early diagnosis applications in Turkish women aged 50 and over. Asian Pacific Journal of Cancer Prevention.
2013;
14
:
5877-82
.
View Article PubMed Google Scholar -
null
null.
International Agency for Research on Cancer; 2013. [7 July 2015]. GLOBOCAN 2012 v1.0, Cancer Incidence Mortality Worldwide: IARC CancerBase, No. 11. [Internet] 2013.
2013
.
-
CM
Gonzaga,
R
Freitas-Junior,
MP
Curado,
AL
Sousa,
JA
Souza-Neto,
MR
Souza.
Temporal trends in female breast cancer mortality in Brazil and correlations with social inequalities: ecological time-series study. BMC Public Health.
2015;
15
:
96
.
View Article PubMed PMC Google Scholar
Comments

Downloads
Article Details
Volume & Issue : Vol 5 No 4 (2018)
Page No.: 2174-2186
Published on: 2018-04-22
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 3836 times
- Download PDF downloaded - 1184 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}