

Evaluation of butyrylcholinesterase and acetylcholinesterase activity in serum and saliva of myocardial infarction patients
- Department of Oral and Maxillofacial Medicine, School of Dentistry, Kermanshah University of Medical Sciences, Kermanshah, Iran
- Students Research Committee, Kermanshah University of Medical Sciences, Kermanshah, Iran
- Department of Clinical Biochemistry, Kermanshah University of Medical Sciences, Kermanshah, Iran
- Medical Biology Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
Abstract
Background: Myocardial infarction (MI) is one of the most common cardiovascular diseases. It accounts for about half of death cases in Iran. The objective of this study was to compare the activity of butyrylcholinesterase (BChE) and acetylcholinesterase (AChE) enzymes in serum and saliva of the MI patients compared to the healthy controls.
Methods: Serum and salivary BChE and AChE levels were measured immediately following MI, and then 24 and 72 hours later. Four mL of blood and two mL saliva were collected for this purpose. These measurements were also collected in 30 healthy controls. The enzymes were assayed using spectrophotometry.
Results: The activity of salivary AChE in the MI patients was lower than that of the healthy controls right after, 24 hours, and 72 hours following MI. However, serum AChE did not show a significant difference between the two groups. The activity of serum BChE in the MI patients was lower than that of the healthy controls right after, 24 hours, and 72 hours following MI. However, salivary BChE did not show a significant difference between the two groups.
Conclusion: The activity of salivary AChE decreased in the MI patients compared to the healthy controls, which can be a marker to diagnose MI in the future.
Introduction
Myocardial infarction (MI) is the permanent and irreversible death of myocytes that is caused by ischemia induced by the blockage in the blood supply into the affected region 1. In an MI attack, about one billion myocytes are destroyed which causes serious complications for cardiac function 1. Cardiovascular diseases are responsible for one-third of all mortalities in the US in 2008 23. Just in the US in 2004, more than 150,000 people died due to MI 4. In addition, MI is also a huge cost burden on healthcare systems 5. In Iran, 50% of all deaths are due to coronary artery disease (CAD), and evidence shows that the prevalence of CAD is increasing 6. The World Health Organization (WHO) estimates that the prevalence of this disease is twice higher in males than in females 7. CAD risk factors are lifestyle-related factors such as smoking, obesity, occupational stress 8910, air pollution 11, poor socioeconomic status 12, diabetes 13, male gender, family history and, age 1415.
Considering the high prevalence of cardiovascular diseases, a detailed and comprehensive understanding of these diseases is highly necessary. Acetylcholinesterase (AChE) enzyme activity in the serum and saliva is one of the factors that have been studied to diagnose MI. Live cells have enzymes and proteins such as creatine kinase, troponin, and myoglobin. When a myocyte dies, the cell membrane loses its integrity, and therefore enzymes and proteins are released into the circulation gradually. These enzymes and proteins can be detected by laboratory methods 1617. Acetylcholine is a neurotransmitter which, via the parasympathetic system, exerts inhibitory effects on the cardiac muscle and results in decreased excitability and increased resting membrane potential. In fact, functions of the cardiovascular system are significantly affected by the autonomic nervous system. Any abnormality in the function of this system due to pathologic conditions such as MI can result in increased cardiac arrhythmia 18. Previous studies demonstrated that low plasma butyrylcholinesterase (BChE) activity might be related to decreased cardiac function 19. Low serum BChE activity is a prognostic marker of mortality associated with poor cardiac functions in acute myocardial infarction 20. In another study, Sulzgruber et al. 21 reported that BChE is a strong predictor for cardiac mortality specifically in younger patients with acute coronary syndrome aged between 45 and 64 years and BChE predicts cardiac mortality in young patients with the acute coronary syndrome. Best of our knowledge, the current study is the first to compare the serum and salivary AChE and BChE activity between MI patients and the healthy subjects. Herein, we decided to compare serum and salivary AChE and BChE activity between myocardial infarction and the healthy controls.
Methods
This study was conducted in the University Hospital and was approved by the Ethics Committee of Kermanshah University of Medical Sciences, Kermanshah, Iran. Two groups were included (the MI group consisting of patients whose diagnosis was confirmed by board-certified cardiologists at the referral cardiology hospital and the control group consisting of healthy people without MI history). The control group was matched regarding age and gender to the MI group. In addition, the MI patients had no history of hemorrhagic stroke, neurologic disease, congestive heart failure, renal failure, hypothyroidism, severe asthma, and sepsis as case group.
Samples Collection
The peripheral blood samples were obtained from the brachial vein (4 mL) and were collected in Falcon tubes containing 0.025M EDTA. Then, the samples were centrifuged at 14000 rpm for five minutes, and the isolated serum was immediately frozen at -45 C. Unstimulated saliva samples were collected in the morning (8 am to 10 am). 2 ml of saliva was collected in five minutes, while the subjects had not drunk any water, nor eaten any food and had not smoked about two hours before sampling. Before sampling, the subjects thoroughly washed their mouth, and after several minutes saliva was collected into Falcon tubes. Then, the samples were centrifuged at 20.000 rpm for 2-3 minutes, and the isolated transparent supernatants were immediately frozen at -45 ºC.
Serum and salivary BChE measurement
Firstly, serum and saliva samples were diluted (1:100) with 133 mM phosphate buffer. For the test tube, 1 mL of distilled water and 2 mL of diluted saliva or serum sample was mixed with 1 mL of 200 mM benzoylcholine chloride. In the blank tube, equal volumes of distilled water and serum or diluted saliva were added. The light absorbance at the wavelength of 240 nm at 25°C was measured after subtracting the absorbance of the blank tubes. Each sample was read five times in a five-minute period (every minute, one absorption). When benzoyl choline (200 nM) is hydrolyzed in a total volume of 4mL and the absorption changes are ∆A= 0.33, the serum and salivary BChE activity was calculated using the following formula:
The normal value of this enzyme is 0.6-1/Uk4/1 (at 25°C) and 1.08-1/Uk 4/2 (at 37C). The additional details (chemicals, kits, instruments, etc.) were reported in the studies of Shahmohamadnejad et al. 22 and Haghnazari et al.23.
Serum and salivary AChE measurement
Firstly, 100 landa of whole blood was irrigated with saline buffer for three times in a glass tube. After irrigation, the sample was centrifuged, and the supernatant was removed, and saline buffer was added. When irrigation finished, the supernatant was removed totally, and 10 mL of 50 mM phosphate buffer was added. Then, in two cuvets (one for the test tube and one for the blank tube), 2 mL of DTNB was added. Then, 1 mL of cellular suspension was added to each cuvet and stored at 30C. After 3 minutes, 100 landa of the substrate was added to the cuvet containing the sample. At wavelength 412 nm, light absorbance of the sample and blank tube were measured. Test tubes were read in a 5-min interval (one reading for every minute). Using the following formula, salivary and serum AChE activity was calculated:
The normal value of the enzyme is 8-1/Uk 13.
Statistical analyses
Descriptive indices including frequency, percentage, mean and its standard deviation (SD) were used to express data. To determine the normal distribution of the data, the Kolmogorov-Smirnov (KS) test was used. To compare the enzyme values between different time points (i.e., immediately following MI, and hours 24 and 72 post-MI), repeated measures analysis of variance (ANOVA) was used. Whenever Mauchly’s test of sphericity was statistically significant, the Greenhouse-Geisser test was applied. For paired comparisons, the Bonferroni’s test was applied. For comparison of the variables between the MI and control groups, the independent sample T-test was used. To determine the correlation between serum and salivary enzyme measurements, the Pearson correlation test was used. The analyses were done by SPSS software (ver. 18.0). The significance level was set at less than 0.05.
Results
There were 30 patients in the MI group and 30 subjects in the control group. In each group, there were 25 males (83.3%) and 5 females (16.7%). The mean (±SD) of ages in the MI and control groups were 52.37 (±6.42) and 50.73 (±7.36) years respectively; P= 0.364. The KS test showed that the variables had a normal distribution (P> 0.05).
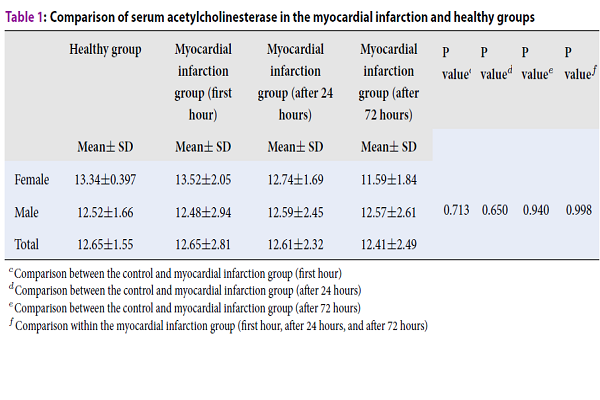
The mean serum AChE levels immediately following MI, 24 hours and 72 hours post-MI were 12.65, 12.61, and 12.41, respectively (
Comparison of serum acetylcholinesterase in the myocardial infarction and healthy groups
| Healthy group | Myocardial infarction group (first hour) | Myocardial infarction group (after 24 hours) | Myocardial infarction group (after 72 hours) | P valuec | P valued | P valuee | P valuef | |
| Mean± SD | Mean± SD | Mean± SD | Mean± SD | |||||
| Female | 13.34±0.397 | 13.52±2.05 | 12.74±1.69 | 11.59±1.84 | 0.713 | 0.650 | 0.940 | 0.998 |
| Male | 12.52±1.66 | 12.48±2.94 | 12.59±2.45 | 12.57±2.61 | ||||
| Total | 12.65±1.55 | 12.65±2.81 | 12.61±2.32 | 12.41±2.49 |
As seen in
Comparison of salivary acetylcholinesterase between control and myocardial infarction groups
| Healthy control | Myocardial infarction group (first hour) | Myocardial infarction group (after 24 hours) | Mmyocardial infarction group (after 72 hours) | P valuec | P valued | P valuee | P valuef | |
| Mean± SD | Mean± SD | Mean± SD | Mean± SD | |||||
| Female | 0.688±0.127 | 0.478±0.155 | 0.410±0.163 | 0.452±0.133 | < 0.001 | < 0.001 | < 0.001 | 0.480 |
| Male | 0.596±0.241 | 0.392±0.185 | 0.439±0.178 | 0.425±0.191 | ||||
| Total | 0.611±0.227 | 0.406±0.151 | 0.434±0.174 | 0.429±0.181 |
There were significant differences in the serum BChE level between the control and MI groups immediately following MI, 24 hours and 72 hours post-MI (P=0.003, P=0.008, and P=0.002, respectively). Repeated measures ANOVA did not show significant changes regarding serum BChE at the three time points (P= 0.794); (
Comparison of serum butyrylcholinesterase between the control and myocardial infarction groups
| Healthy control | Myocardial infarction group (first hour) | Myocardial infarction group (after 24 hours) | Myocardial infarction group (after 72 hours) | P valuec | P valued | P valuee | P valuef | |
| Mean± SD | Mean± SD | Mean± SD | Mean± SD | |||||
| Female | 2.46±0.329 | 1.84±0.654 | 2.44±0.434 | 1.98±0.722 | 0.003 | 0.008 | 0.002 | 0.794 |
| Male | 2.37±0.577 | 1.83±0.847 | 1.81±0.775 | 1.85±0.666 | ||||
| Total | 2.39±0.540 | 1.83±0.808 | 1.92±0.761 | 1.87±0.664 |
As seen in
Comparison of salivary butyrylcholinesterase between the control and myocardial infarction groups
| Healthy control | Myocardial infarction group (first hour) | Myocardial infarction group (after 24 hours) | Myocardial infarction group (after 72 hours) | P-valuec | P-valued | P-valuee | P-valuef | |
| Mean± SD | Mean± SD | Mean± SD | Mean± SD | |||||
| Female | 0.003±0.002 | 0.004±0.002 | 0.003±0.002 | 0.002±0.002 | 0.827 | 0.752 | 0.097 | 0.049 |
| Male | 0.003±0.002 | 0.003±0.002 | 0.003±0.002 | 0.002±0.001 | ||||
| Total | 0.003±0.002 | 0.003 ±0.002 | 0.003 ±0.002 | 0.002 ±0.001 |
There was no significant correlation between the serum and salivary level of AChE immediately following MI (r= 0.08, P= 0.676), 24 hours after MI (r= 0.017, P= 0.929), and 72 hours after MI (r= 0.141, P= 0.457). No significant correlation existed between the salivary and serum level of AChE in the control group (r= 0.301, P= 0.106). Also, no significant correlation was found between the salivary and serum level of BChE immediately after MI (r= 0.233, P= 0.242), 24 hours after MI (r= 0.06, P= 0.771), and 72 hours after MI (r= 0.105, P= 0.642). No significant correlation existed between the salivary and serum level of BChE in the control group (r= 0.356, P= 0.054).
Discussion
Acetylcholine is the main neurotransmitter of the parasympathetic system, and its level is regulated by AChE and BChE through hydrolysis 242526. This study investigated the activity of AChE and BChE enzymes in the saliva and serum in patients with MI in comparison to healthy subjects to identify markers to diagnose of MI. MI is one of the common cardiac conditions 27, and its main cause is atherosclerosis. One study 28 reported that serum AChE and BChE levels decreased following MI. The activity of these enzymes can be important in the development of MI and also be protective. Clinical findings and electrocardiography do not achieve the required sensitivity and specificity 28. The measurement of these enzymes can be useful in managing patients suspected to suffer MI. A limited number of studies has been performed regarding the activity of AChE and BChE in the MI patients 2927. One of the quick, cost-effective, and non-invasive methods for MI diagnosis could be the measurement of AChE and BChE activity in the serum and saliva. The previous studies have not been determined the changes in the activity of these enzymes in the saliva and serum of MI patients.
This study showed a significant decrease of AChE levels in the saliva of the MI patients compared to the control group immediately following MI, 24 hours and 72 hours post MI. We did not find any similar study in the literature assessing the salivary AChE and BChE levels in the MI patients. In a study by Mirzaii‐Dizgah et al. 30 including 30 salivary samples of patients with acute MI and 28 healthy subjects, salivary troponin level, as a marker for the diagnosis of MI, was higher in the MI patients than in the control group at 12 and 24 hours after MI. The observed findings in this study and increased salivary troponin levels in the mentioned study 30 showed increased cardiac-related enzymes following MI. Our results showed decreased serum BChE levels in the MI group immediately following MI, 24 hours and 72 hours post MI. In a previous study, it was reported that MI patients with reduced BChE levels experienced a higher mortality rate 29. As AChE and BChE enzymes are synthesized in cardiac muscle, their levels decrease after MI. This study is the first to investigate AChE and BChE serum and saliva levels in MI patients compared to the controls. During necrosis of myocardium, the AchE released by injury of cholinergic nerve and AchE can be a parameter for MI diagnosis.
Conclusions
Our findings showed a significant reduction in salivary AChE and serum BChE in the MI group in comparison to the control group. As the main objective of this study was to measure these two enzymes following MI, the results suggest that salivary AChE can be used as a marker the to diagnose MI in the future. As this study was done for the first time, we suggested that further studies with a larger number of salivary samples and for longer follow-up times be performed in the future. With such studies, the definitive role of AChE and BChE in diagnosing and managing MI patients will be validated.
Competing Interests
Authors have no conflict of interest.
Authors' Contributions
Neda Omidpanah: Design of the study and acquisition of data.
Negin Jalilian: Collection of data
Asad Vaisi-Raygani: Analysis and interpretation of data.
Masoud Sadeghi: Revision of the article and final approval of the version to be published.
Hamid Reza Mozaffari: Writing of the article.
Acknowledgments
This paper is issued from the thesis of Negin Jalilian and financial support was provided by Kermanshah University of Medical Sciences (Project code: 95336).
List of abbreviations
MI: Myocardial infarction
BChE: Butyrylcholinesterase
AChE: Acetylcholinesterase
CAD: Coronary artery disease
SD: Standard deviation
KS: Kolmogorov-Smirnov